Dental Caries: The disease and Its Clinical Management
Part II Clinical caries epidemiology
P123
8 The epidemiology of dental caries
8章 齲蝕の疫学
B. A. Burt, V. Baelum and O. Fejerskov
P123-45
Introduction
導入
Measuring dental caries
齲蝕を評価する
Distribution of caries
齲蝕の分布
Summary
まとめ
References
P124
Introduction
導入
Epidemiology is the study of health and disease in populations, and of how these states are influenced by heredity, biology, physical environment, social environment and human behavior.
疫学は、集団における健康と疾病を、また、これらの状況は
遺伝的生物的物理的環境、社会的環境、人間の行動から、どのような影響を受けているのかを研究する分野である。
It differs from clinical studies in that epidemiology’s focus is on groups of people, often whole populations, rather than on individuals or patients.
疫学と臨床研究の違いは、疫学は個人や何人かの患者ではなく、人々の集団、しばしば母集団に焦点を絞るということにある。
The goal of epidemiological study is to identify the risk of disease that follows certain exposures, so that appropriate preventive interventions may be carried out at the public health and individual levels.
疫学研究の目標は、適切な予防介入が公衆衛生と個人水準で実行できるように、特定の暴露に続いて生じる疾病のリスクを特定することにある。
To achieve this goal, epidemiological study uses a number of different research designs.
この目標を達成するために、疫学研究は、さまざまな研究デザインを利用する。
All of them, however, include people with and without the disease in question, and with and without exposure to the correlates of interest.
しかし、あらゆる研究デザインは、対象となっている疾病のある人々とない人々、また関心を引く相互に関連のあるものへの暴露のある人々とない人々からなる。
 While research designs can become quite involved, Figure 8.1 shows the simple matrix that is the core of all epidemiological investigations.
While research designs can become quite involved, Figure 8.1 shows the simple matrix that is the core of all epidemiological investigations.
研究デザインはかなり複雑となりうるが、Figure 8.1に、あらゆる疫学研究の中核をなす簡単なマトリックスを示す。[2010.1.29]
Many factors are considered to be part of the causal chain in dental caries: bacteria, diet, plaque deposits, saliva quantity and quality, enamel quality, genetic history and tooth morphology have all been studied as possible risk factors for caries (Chapter 29).
多くのファクターが、齲蝕における因果連鎖の一部であると考えられている。齲蝕のリスクファクターの可能性を秘める細菌、食糧、プラークの堆積、唾液の質と量、エナメル質の質、遺伝的経歴と歯の形態のすべてが、研究されている (Chapter 29)。
A risk factor is defined as:
リスクファクターは、以下のように定義される。
An environmental, behavioral, or biologic factor confirmed by temporal sequence, usually in longitudinal studies, which if present directly increases the probability of a disease occurring , and if absent or removed reduces the probability.
その存在が疾病発生の可能性を直接に増加させ、そしてそれが欠如または取り除かれると可能性が減少することを、通常は縦断研究により、時間的順序に確認された、環境的行動的生物的ファクター。
Risk factors are part of the causal chain, or expose the host to the causal chain.
リスクファクターは因果連鎖の一部であるか、宿主を因果連鎖にさらす。
Once disease occurs, removal of the risk factor may not result in a cure (Beck, 1998).
いったん疾病が生じれば、リスクファクターを取り除いても、治癒にはいたらないこともある (Beck, 1998)。
Epidemiology’s role is to identify the risk factors for disease.
疫学の役割は、[集団における]疾病のリスクファクターの特定にある。
As stated in the definition above determining whetherexposure to a potential risk factor leads to a particular disease requires longitudinal study.
上記の定義に述べられている通り、リスクファクターと見込まれるものへの暴露が特定の疾病につながるかどうか、を判断するには、縦断研究が必要である。
Where there is evidence to suggest that a particular exposure is a risk factor, but the relationship cannot be confirmed through prospective study, the exposure is referred to as a risk indicator.
ある暴露がリスクファクターであると示唆する検証があり、しかしその関係が前向き研究により確認出来ない場合は、その暴露はリスクインディケーターと呼ばれる。
Major intraoral entities that are part of the causal chain (e.g. oral microflora, specific dental plaques, and saliva quality and quantity) are dealt with in detail elsewhere in this book and so will not be part of this chapter.
(口内微生物叢、特定のデンタルプラーク、唾液の質と量といった)因果連鎖の一部である主要な口内に存在する物については、他の章に詳しいため、本章では扱わない。
Instead, the distribution of dental caries in populations, and the factors that influence that distribution, are examined here.
代わりに、集団における齲蝕の分布とその分布に影響を与えるファクターを精査する。
A major theme is that severe caries today is increasing ly being recognized as a disease that closely follows a social gradient, so this chapter is broadened to emphasize the important role of the social environment in caries distribution.
重度の齲蝕は、今日ますます、社会的勾配に忠実に従う疾病であると認識されてきており、そこで本章は、齲蝕の分布における社会的環境の役割の重要性をひもとく。[2010.1.30]
After a brief look at some of the issues in caries measurement, the relationships between caries experience and national income levels (as a broad measure of social resources) are examined.
齲蝕の評価におけるいくつかの課題を確認した後、齲蝕経験と(社会資源の指標として)国家の収入水準の関係を調べる。
Then, following a brief consideration of how caries distribution is related to those individual attributes that cannot be changed, e.g. age, race, gender and genetic predisposition, the relationship between caries and socioeconomic status (an individual measure) and social determinants (a community measure) is explored.
そして、齲蝕の分布が、年齢、人種、性別、疾病についての遺伝的素質といった変えることのできない個人的特性に、どれほど関連しているのかを考察し、齲蝕と(個人の指標である)社会経済的地位、そして(地域の指標である)社会的決定要因の関係を検討する。[SESは個人の行動の要約指標、social determinantsは地域のヘルスアウトカムに影響を与えるファクター]
These community-based factors, sometimes called neighborhood characteristics, are now recognized as having a strong influence on caries extent and severity.
近隣特性とよばれるこれらの地域単位のファクターは、近年、齲蝕の広がりと重症度に大きな影響をもたらしている、と認識されている。[multi level analysisのことか?]
Caries is an ancient disease
古代からの病、齲蝕
Dental caries has been making people miserable since at least the time when humans began to develop agriculture.
齲蝕は、少なくとも、人類が農耕を始めるころには、人々を蝕んでいた。
From palentological remains from the Iron Age, it appears that carious lesions in young people sometimes began in occlusal fissures, but developed no further because attrition progressed faster than caries.
鉄器時代の旧人類の遺骨からは、しばしば咬合面裂溝にはじまる齲蝕病巣が認められているが、齲蝕より磨耗の進行する速度の方が上回っていたため、齲蝕がそれ以上進行している様子は認められていない。
This pattern of development can still be seen today, e.g. in some African populations, where the rate of progression on approximal surfaces may also be so low that these lesions are ground away.
アフリカの一部では、今日でもこの傾向が見られるが、隣接面の進行速度も遅いため、齲蝕病巣は磨滅してしまう。
Most lesions found in human remains from the Iron Age were cervical or root caries; coronal caries was relatively uncommon at this time, although it became more common during the time of the Roman Empire.
鉄器時代の人骨の齲蝕病巣の大部分は、歯頚部ないし根面に認められる。歯冠齲蝕は、この時代では比較的蔓延していなかったのだろう。しかし、古代ローマ帝国時代には、歯冠齲蝕は猛威を振るうことになった。
Roman remains give evidence that some teeth with large coronal cavities had obviously been treated.
ローマ人の遺骨には、明らかに治療をしたと思われる、大きな歯冠齲蝕の痕跡がみられる。
The moderate caries experience found in Britain during the Anglo-Saxon period (sixth to seventh centuries) had changed little by the end of the Middle Ages (Moore & Corbett, 1971, 1973).
イギリスでは、アングロサクソン時代(16-17世紀)から中世の終焉まで、齲蝕の蔓延の程度は、中等度のままで、ほとんど変化がなかった (Moore & Corbett, 1971, 1973)。
Increased consumption of processed food and greater availability of sugar were probably chiefly responsible for the development of the modern pattern of caries.
現代の齲蝕の傾向は、主に、加工食品の消費の増大と砂糖の普及に原因がある。[2010.2.2]
Import duties on sugar in Britain were relaxed in 1845 and completely removed by 1875, a period during which the severity of caries increased greatly (Corbett & Moore, 1976; Lennon et al., 1974).
イギリスの砂糖の輸入税は1845年から緩和され、1875年には完全に撤廃された。齲蝕の時代の始まりである (Corbett & Moore, 1976; Lennon et al., 1974)。
By the end of the nineteenth century, dental caries was well established as an epidemic disease of massive proportions in most of the economically developed countries (Burt, 1978).
19世紀末までに、経済発展を遂げた国々の多くで、齲蝕は地域的疾病の地位を確立していた (Burt, 1978)。
The severity of the caries epidemic in the late nineteenth century led directly to the establishment of public dental services, which first appeared in the Scandinavian countries.
19世紀末には、齲蝕の地域的流行の厳しさは、公的歯科医療の設立へとつながった。スカンジナビア諸国でのことである。
P125
Measuring dental caries
齲蝕の評価
To study caries and its distribution in populations, it must be possible to measure it validly and reliably, and then put those measurements together in some systematic fashion so that caries distribution in one group can be compared with that in another.
齲蝕と集団におけるその分布を研究するためには、ある集団における齲蝕の分布と他の集団における齲蝕の分布を比較できるように、妥当性と信頼性のある齲蝕の評価とその評価の体系化が必要である。
Since the disease of dental caries occurs on a continuum, from the earliest demineralization to cavitation, it is clearly important to have clear rules, or criteria, for the conditions under which caries is judged to be present.
齲蝕は、脱灰初期から齲窩にいたるまで連続的に生じるため、それが齲蝕なのかどうか、はっきりとした規定や基準を設けることは、重要である。
(Chapter 9 shows the impact of using differing measurement criteria on prevalence and severity data).
(評価基準のばらつきが、有病割合と重症度の資料にもたらす影響については、9章に詳しい)
Valid and reliable measurement is the basis of any science, including epidemiology, where an index (a numerical scale with upper and lower limits, with scores on the scale that correspond to specific criteria) is usually required to obtain a precise expression of disease distribution in a group.
妥当性と信頼性の評価は、ありとあらゆる科学の基本であり、とりわけ疫学では、指数(特定の基準に一致する尺度に基づくスコアで上限と下限のある数値指標)は、通常集団における疾病の分布を明瞭に説明することを要求される。
The properties of an ideal index are listed in Box 8.1.
理想的な指数の性質をBox 8.1に掲げる。
Index scores usually give no picture of clinical conditions (e.g. what does a plaque index score of 1.2 look like?), and in the past were often statistically mistreated when averages were computed from ordinal scales, but they have value when compared with the index scores from other groups measured in a similar way.
指数スコアは、通常臨床的状況を表さず(たとえば、プラーク指数1.2とは?)、また過去には順序尺度から平均を算出するなど、しばしば統計的に誤って処理されていた。しかし、指数スコアは、似た方法で評価されたほかの集団の指数スコアと比較する場合には、価値がある。[2010.2.3]
While various indexes for measuring caries were suggested during the 1920s to the early 1930s, it was only with Dean’s studies of naturally occurring fluoridated water in the 1930s that a practical method was developed and used.
1920年代から1930年代初頭にかけて、齲蝕を評価するためのさまざまな指数が提案され、実用的方法が開発、利用された1930年代には、Deanによる天然水中のフッ化物の研究が行われた。
Dean and his colleagues (Dean et al., 1942) counted the numbers of teeth in the mouth with obvious caries (i.e. cavities).
Deanとその同僚は、あきらかな齲蝕(すなわち齲窩)の歯の本数を数えた (Dean et al., 1942)。
Filled teeth and teeth missing due to caries were added in, so that the index score included all teeth that had been attacked by caries.
齲蝕の影響を受けたすべての歯を指数スコアに反映させるため、齲蝕のために充填した歯と喪失歯も加算した。
The first description of what is now known as the DMF index came from extensive studies of dental caries among children in Hagerstown, Maryland, USA, in the 1930s (Klein et al., 1938).
現在、DMF指数として知られているものが最初に記述されたのは、1930年代、USAのMaryland州Hagerstownの小児の齲蝕の大規模な調査である (Klein et al., 1938)。
After that, the DMF index became the most used of all dental indexes.
その後、DMF指数は、齲蝕の指数の中では、最もよく利用される指数としての地位を確立した。[2010.2.4]
The DMF index
DMF指数
As originally described, D was for decayed teeth, M for teeth missing due to caries and F for teeth that had been previously filled.
もともとは、Dは齲歯、Mは齲蝕による喪失歯、Fは充填歯のことであった。
Filled teeth were assumed to have been unequivocally decayed before restoration.
充填歯は、修復される前には間違いなく齲蝕であった、と仮定していたのである。
The index could be applied to teeth as a whole (designated as DMFT), or applied to all surfaces of the teeth (DMFS).
この指数は、すべての歯 (DMFT)、ないし歯面 (DMFS) に適応される。
The DMFT score for anyone individual can range from 0 to 32, in whole numbers, while the mean DMFT score for a group can have decimal values.
個人のDMFTスコアは0-32の整数となるが、集団のDMFTスコアの平均値は小数値となる。
The index can be modified to deal with such factors as filled teeth that have redecayed, crowns, bridge pontics and any other particular attribute required for study.
この指数は、改変され、二次齲蝕、クラウン、ポンティック、研究に必要なその他の属性といった要素を充填歯として扱う。
It can also be applied with varying criteria for what constitutes caries.
DMF指数は、齲蝕を構成する、さまざまな基準にも適応される。
The original intention to scored only when there was cavitation has largely given way to scoring systems which record caries at all stages from the earliest enamel caries through to cavitation.
齲窩のある時のみカウントするという、もともとの意図は、初期エナメル質齲蝕から齲窩までのすべての段階を齲蝕として記録する、スコアリング体系に取って代わられてきている。
An example of the latter is the International Caries Detection and Assessment System (ICDAS), which records caries on a six-point ordinal scale (Pitts, 2004).
後者の例には、国際齲蝕検出評価体系 (ICDAS) があり、これは齲蝕を6点の順序尺度で記録する (Pitts, 2004)。
An otherexample is a scale that disting uishes between caries progress in active and inactive lesions (Nyvad et al., 1999).
その他には、進行性と非進行性の齲蝕を区別する基準がある (Nyvad et al., 1999)。
As a result, DMF scores where caries is measured over its full range of development are higher than those where only cavitation, i.e. a later stage of caries progression, is used as the criterion for decayed teeth.
結果として、DMFスコアは、齲窩のみをカウントする場合よりも、あらゆる進行をカウントする場合の方が大きくなる。
The DMF index has been used widely since its introduction in 1938 because it meets a number of the criteria for an ideal index (Box 8.1).
DMF指数は、1938年に導入されて以来、幅広く利用されている。というのは、この指数は理想的指数の基準を数多く満たしているからである (Box 8.1)。
For example, it is simple, versatile, statistically manageable and reliable when examiners have been trained.
例えば、DMF指数は、簡単で、融通が利き、統計的に扱いやすく、検査員が訓練を受けていれば、信頼性がある。
However, the DMF does have its limitations, and the main ones are listed in Box 8.2.
しかし、DMFには欠点もある。主なものをBox 8.2に示した。
The limitations of the DMF index today frequently relate to moden preventive and restorative technology.
DMF指数の欠点は、今日の予防、修復技術としばしば関連している。
For example, there were no sealants or adhesive resins when the DMF index was first developed.
例えば、DMF指数が開発された頃には、シーラントも接着樹脂も開発されていなかった。
There are two reasonable approaches for adapting the DMF to deal with sealants.
DMFをシーラントに適応させるための、2つの妥当な手法がある。
One says that the sealed tooth is not restored in the usual sense and should therefore be considered sound.
1つは、シーラント歯は通常、充填ではなく、健全であるをみなすべきである、というものである。
The other says that it has required hands-on, one-to-one dental attention, and so should be considered a filled tooth.
もう1つは、シーラントには歯科診療が必要であり、充填歯とみなすべきである、というものである。
Probably the best way to deal with sealed teeth is to put them in a category by themselves, S for sealed.
たいていシーラント歯を扱う最良の方法は、シーラントを示す、Sという分類を作ってしまうことである。
The DMFS index would then become DMFSS.
DMFS指数は、DMFSSになる。
Depending on the study’s purpose, thes teeth can be left separate, included with for regarded as sound.
S歯は、Fに含まれるか、健全歯とみなされるが、研究の目的によっては分けられたままとなる。
The DMF index today is really out dated as a measure of caries incidence and severity, and may actually be more valid as a measure of treatment received.
DMF指数は、今日、齲蝕の発生数と重症度の指標としては、実際のところ時代遅れであり、また、受療の評価としては、わりと妥当である。[2010.2.5]
It is philosophically questionable to use an index for a disease that is so dependent upon the treatment judgments of many practitioners, and the combination of previous treatment (i.e. the M and F components) with current treatment need (the D component) is not used elsewhere in public health surveillance.
多くの臨床家の治療判断に大きく依存する疾病の指数を利用することは、哲学的に疑問であり、以前の治療 (M, F) と現在の治療ニーズ (D) の組み合わせは、他の公衆衛生調査では利用されていない。
An objective measure of caries activity (e.g. a marker of active disease) would be preferable to clinical judgment for many purposes, but because valid markers for caries are elusive, scoring caries activity is still based on clinical acumen (Nyvad et al., 1999).
齲蝕活動性の客観的評価(たとえば、活動性疾病マーカー)は、さまざまな目的の臨床判断で好まれるが、齲蝕の妥当なマーカーはエルーシブなため、現状、齲蝕活動性のスコアリングは臨床的洞察に基づいている (Nyvad et al., 1999)。
On the credit side DMF has been used for generations and still has some use in monitoring trends over time.
DMFは長年にわたり利用されてきており、いまだに経年的な傾向の把握に利用されている。
Its mix of treated and untreated caries measures also gives it some value in health services research.
未治療齲蝕と治療済み齲蝕の評価を、組み合わせることは、医療の研究においても、価値がある。
Until a more objective measure is developed and accepted then some modification of DMF will continue to be the principal index used to express the caries status of a population.
より客観的な評価が開発され、普及するまでは、改変DMFが、集団の齲蝕状況を表現する指数の第一選択であり続けそうだ。[2010.2.6]
P126
Other measures of caries
齲蝕のその他の評価
Other methods of measuring dental caries, using different philosophical bases, have been suggested from time to time.
ときどき、DMFとは異なる哲学に基づいた齲蝕を評価する方法が提案される。
One is Grainger’s hierarchy, an ordinal scale designed to simplify the recording of the caries status of a population, which uses five zones of severity of the carious attack (Grainger, 1967).
その1つがGraingerのヒエラルキーであり、これは集団における齲蝕の状況の記録を単純にする順序尺度であり、齲蝕の重症度を5つのゾーンで考える (Grainger, 1967)。
This method was based on a landmark paper of Klein and Palmer (1941), which presented a caries susceptibility order for the teeth, an ordering which has changed little down the years (Macek et al., 2003).
Graingerのヒエラルキーは、KleinとPalmer (1941) の有名な論文に基づいており、歯の齲蝕感受性の序列を示し、その序列は昔からほとんど変わっていない (Macek et al., 2003)。
Several studies confirmed the validity of the hierarchy (Katz & Meskin, 1976; King man, 1979; Poulsen & Horowitz, 1974).
多くの研究が、このヒエラルキーの妥当性を確認している (Katz & Meskin, 1976; King man, 1979; Poulsen & Horowitz, 1974)。
The Grainger hierarchy could be useful in public health surveillance, but it has received little further use.
Graingerのヒエラルキーは、公衆衛生調査では便利であるが、ほとんど使われていない。
‘Composite’ indicators have been suggested that attempt to measure health rather than disease by statistically weighting healthy restored teeth differently from missing or decayed teeth (Sheiham et al., 1987).
‘合成’指標は、喪失歯や齲歯と健康な修復歯の重み付けを統計的にかえることで、疾病ではなく健康を評価しようとしている (Sheiham et al., 1987)。
The first of these is the FS-T, which sums the sound and well-restored teeth.
第1はFS-Tとよばれ、健全歯と修復歯の合計である。[2010.2.8]
The second is T-Health, which seeks to measure the amount of healthy dental tissue and ascribes descending numerical weights for a sound healthy tooth, a well-restored tooth and a decayed tooth.
第2に、健全な歯の組織の量を評価し、また健全歯、修復歯、齲歯の順に数的重みをつける。
These are conceptually sound approaches to measuring dental health and function (rather than disease), and they probably deserve more attention than they have received.
これらは、歯の(疾病ではなく)健康と機能を評価する概念的に健全な手法であり、たぶん現状より評価されるにふさわしいものである。[ん?sheihamに、なにかつかまされたか?]
An offshoot of the present-day skewed distribution of caries is the significant caries index (SiC) (Bratthall, 2000; WHO, 2005).
今日の齲蝕の傾斜分布から派生したのが、SiC指数である (Bratthall, 2000; WHO, 2005)。[正規分布しない状況の要約には、パーセンタイルも推奨されています]
The SiC is not a new index, but rather is a form of data presentation to help give a better picture of caries distribution in the population.
SiCは新しい指数ではなく、集団における齲蝕分布の状況をよりよく示す資料である。
It is the mean DMF score for the third of the population that is most affected by caries, intended to be used along side the mean DMF of the whole population to give a more complete summary of its caries distribution.
SiCは集団の中の齲蝕の多い1/3のDMFスコアの平均値であり、より完全な要約として集団全体のDMFの平均値に添えて利用される。
The more skewed the distribution, the greater the gap between the mean DMF and the SiC.
分布が歪んでいるほど、DMFの平均値とSiCの差は大きくなる。
Criteria for diagnosing coronal caries
歯冠齲蝕の診断基準
There is no global consensus on the criteria for diagnosing dental caries, despite a vast quantity of words on the subject.
齲蝕の診断基準については、大量の言葉が語られているが、その実、国際的基準はない。
Apart from the inherent problem of diagnosing a borderline lesion, the major philosophical issue comes with scoring the early carious lesion which has not yet become cavitated.
境界線直上の病巣の診断につきものの課題は別にしても、まだ齲窩を形成していない初期齲蝕病巣のスコアリングにともなう哲学的課題がある。
These lesions appear as discolored fissures without loss of substance, as a ‘white spot’ on visible smooth surfaces, or radiographically as an early interproximal shadow.
実質欠損のない変色した裂溝、平滑面の‘白斑’、隣接面のレントゲン上の陰影などである。
The issue is that not all non-cavitated lesions progress to dentinal lesions requiring restorative treatment, and active non-cavitated lesions should receive non-operative treatment to prevent any further caries progression.
この課題の核心は、すべての齲窩のない病巣が修復治療の必要な象牙質病巣に進行するわけではなく、また活動性非齲窩性病巣は、齲蝕の進行を妨げるために非外科的治療を受けるべきである、ということにある。
With non-operative treatment (or sometimes even without it), a good proportion of them will remain static or even remineralize (Pitts, 1993).
活動性非齲窩性病巣は、非外科的治療を受ければ(あるいは、なにもしなくても)、そこそこ停止するか、あるいは再石灰化する (Pitts, 1993)。
These lesions arethus reversible, as opposed to dentinall esions, which are usually considered irreversible.
象牙質齲蝕は通常、非可逆性であると考えられているが、これらの病巣は可逆性であるのだ。
Because there are usually more non-cavitated than cavitated lesions at anyone time in both high-caries and low-caries populations (Pitts & Fyffe, 1988; Bjarnason et al., 1992; Ismail et al., 1992; Machiulskiene et al., 1998), the decision of whether to include or exclude them, and how to express them if included, can make a substantial difference in the oral health profiles obtained (Chapter 9).
普通は、いつ、いかなる場所であれ、齲窩のある病巣より、齲窩のない病巣の方が多い (Pitts & Fyffe, 1988; Bjarnason et al., 1992; Ismail et al., 1992; Machiulskiene et al., 1998) ため、齲窩のない病巣を含むか除くかの決断と、もし包含するならそれをどう表すのかは、口内保健の輪郭に相当なずれをもたらす。
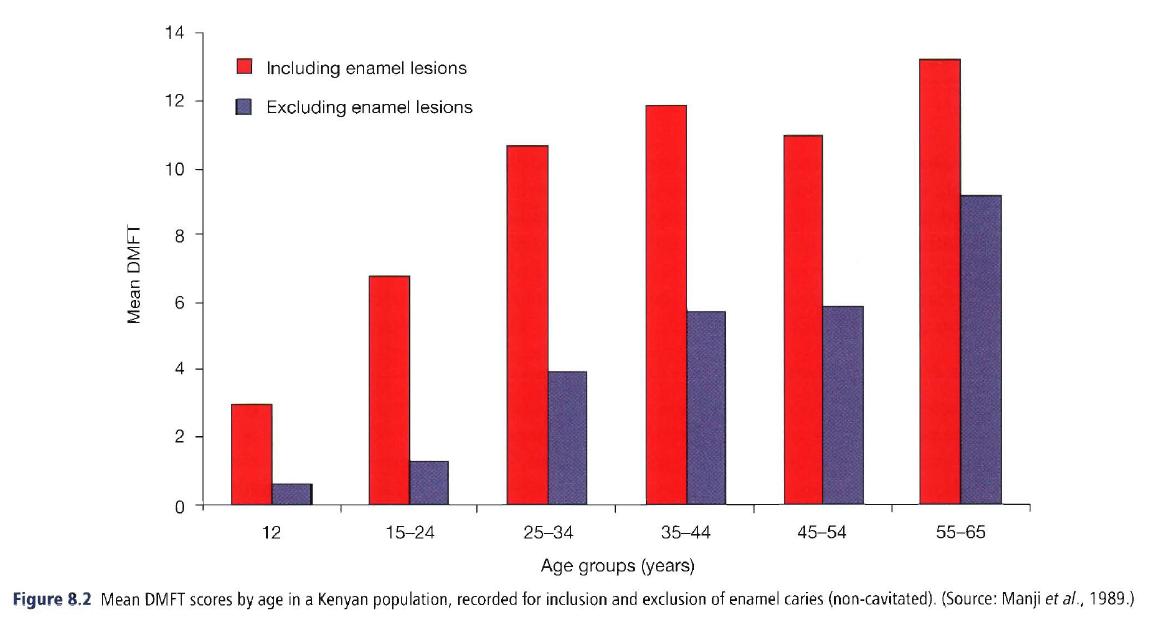 This is illustrated in Fig. 8.2, where in surveys in Kenya the carious lesions were recorded as both cavitated and enamel-only (i.e. non-cavitated).
This is illustrated in Fig. 8.2, where in surveys in Kenya the carious lesions were recorded as both cavitated and enamel-only (i.e. non-cavitated).
齲窩のある齲蝕とエナメル質齲蝕(齲窩のない齲蝕)の両方を記録しているKenyaでの齲蝕の調査をFig. 8.2に示す。[2010.2.11]
There is a marked difference in any caries profile depending on whether non-cavitated lesions are included or not.
齲窩のない齲蝕の含除により、齲蝕の輪郭には相当な違いがある。
P127
Examples of these two broad approaches to diagnostic criteria for dental caries are shown in Box 8.3.
齲蝕の診断基準に対する2つのアプローチの例をBox 8.3に示す。
European investigators have long recorded caries on a scale that extends through the full range of disease from the earliest detectable non-cavitated lesion through to pulpal involvement (Backer Dirks et al., 1961).
欧州の調査員は、最初期検出可能非齲窩性病巣から、歯髄侵襲性齲蝕病巣まで、あらゆる進行段階を評価できる尺度で齲蝕を記録している。
The criteria in Box 8.3 were first published by the World Health Organization (WHO) in 1979 (WHO, 1979), and will be referred to as the D1-D3 scale.
Box 8.3の基準は、1979年にWHOから公表されたもので、D1-D3尺度と呼ばれている。
(There is a D4 for pulpal involvement, but that recording is seldom contentious.)
(D4もあるにはあるが、めったに使われない)
More recently, clinical researchers in Europe have expanded on this concept to produce a scale with up to 10 points, combining increasing depths of lesion development with clinical signs of activity or inactivity (Machiulskiene et al., 1999; Nyvad et al., 1999; Pitts, 2004).
より近年、欧州の臨床研究者は、病巣進行の深さと活動性あるいは非活動性の臨床上のサインを組み合わせて、この尺度を10ポイント制に改変している (Machiulskiene et al., 1999; Nyvad et al., 1999; Pitts, 2004)。[2010.2.12]
However, investigators in North America, Britain and other English-speaking countries have until recently used visual tactile means to record caries as a dichotomous condition, meaning that caries was recorded only as present or absent.
一方、North America、Britain、そのほかの英語圏の検査者は、齲蝕の有無のみを、ななんと、視診と触診に頼って記録している。
(This is referred to here as the dichotomous scale.)
(ここでは、これを、2点尺度[有無のみの評価]と呼ぼう。)
In the dichotomous recording , caries was only noted when it reached the level of dentinal involvement (Horowitz, 1972), i.e. the D3 level.
2点尺度では、齲蝕は象牙質侵襲性(D3)に達したもののみをカウントする (Horowitz, 1972)。
The D1-D3 scale requires the teeth to be dried and receive a longer, more meticulous examination, although with well-trained examiners this can be done even under fairly primitive field conditions.
D1-D3尺度は、歯の乾燥と、長く細やかな診査を必要とするが、よく訓練された検査者であれば、かなり原始的な現場の条件下であっても、判定は可能である。
A scoring system based on the D1-D3 scale is a necessity in cariology research studies, for it permits identification of lesion initiation, progression and regression.
D1-D3尺度に基づいたスコアリング体系は、病巣の初期、進行、逆行を同定できるので、齲蝕研究には不可欠である。
Research questions on the conditions under which early lesions progress, regress or remain static can only be answered with a measurement scale of this nature.
どのような状況下で、初期病巣が進行するのか、逆行するのか、停止するのかという疑問は、この性質をもつ尺度によってのみ、答えられる。
Its use demands meticulous examiner training, since because D1 lesions are capable of remineralizing back to sound enamel it becomes difficult to differentiate examiner error from natural phenomena.
D1病巣は再石灰化して健全なエナメル質になりうるため、検査者による診断の過誤と自然現象を区別するのが困難であることから、D1-D3尺度は、細やかな検査者のトレーニングを要求する。
This may influence the assessment of absolute changes, although in the absence of bias it should not affect the contrast between groups.
これは絶対的な変化の評価に影響するが、バイアスがなければ、集団間の比較[相対的な変化の評価]には影響がない。
There is less consensus on whether the D1-D3 scale should be used in large-scale surveillance surveys, for arguments can be made both ways.
D1-D3尺度と2点尺度[有無のみの評価]、両方について議論があり、D1-D3尺度が大規模な実態調査に使われるべきかどうかについての合意はない。
Surveillance surveys are conducted at multiyear intervals to address the broad questions of whether disease levels are increasing or decreasing so that appropriate public policy can be formulated.
適切な政策を形作るため、疾病水準の上下を把握するため、実態調査は複数年間隔をあけて実施される。
For comparisons over time, it is clear that disease-measurement criteria need to be similar, and generally the simpler the system the better the examiner reliability.
長年の比較のために、疾病の評価基準は類似していている必要があるのは、明らかであり、一般に、体系が単純なほど検査者の信頼性はよくなる。
However, measuring caries only when cavitation can be detected underestimates the true extent of caries.
しかし、齲窩のあるときのみ齲蝕を評価することは、齲蝕の真の広がりを過小評価する。
Some see measuring caries only when cavitation is present as serving to perpetuate the old-fashioned ‘drill-fill-bill’ approach to tooth repair, while others see the opposite, that the same undesirable outcome will come from recording early demineralized lesions that should receive non-operative treatment.
齲窩のあるときのみ齲蝕を評価することは、歯の修復の遺物である‘形成-充填-請求’アプローチの延命であるとする人もいる。また、ある人は、正反対なことに、非外科的治療を受けるべき初期脱灰病巣を記録することは、好ましくない結果が生じる、と懸念する人もいる。
This discussion is likely to continue.
この議論は、続きそうである。
P128
Measuring caries treatment needs
齲蝕治療ニーズの評価
Assessment of the caries treatment needs of a group, at first glance, appears to be nothing more than the segment of a mean DMF score assessed from a survey.
集団の齲蝕治療ニーズの評価は、一見、調査から評価されるDMFスコアの平均値で、こと足りる、ように見える。
This approach, however, has been shown not to work, for the reasons listed in Box 8.4.
しかし、Box 8.4に示すように、このやり方は、うまく機能しないことが、明らかとなっている。[2010.2.13]
Because surveys are usually conducted in field conditions that are less than ideal, relative to the dental office, it would be expected that surveys detect fewer carious lesions than practitioners do.
調査は通常、歯科診療所と比較して、理想的とは言いがたい状況で実施されるため、検出される齲蝕の数は、診療所で行われるよりも少なくなると思われる。
However, that begs the question of which assessment is ‘correct’.
しかし、これは、どのような評価が‘正しい’のかという疑問に帰結する。
Field surveys can miss early lesions, but practitioners can also overtreat.
現地調査は、初期病巣を見逃すかもだが、臨床医は過剰治療するかも、なのである。
To add to the uncertainty, treatment plans for the same patients have been shown to vary drastically from one dentist to another (Espelid et al., 1985; Bader et al., 1993; Nuttall et al., 1993).
この不確実性に加えて、同じ患者でも、歯科医師により治療計画は大きく異なることが、示されている (Espelid et al., 1985; Bader et al., 1993; Nuttall et al., 1993)。
The difficulty of determining treatment needs by survey was illustrated after a 1978 national dental survey in Britain.
調査により治療ニーズを決定することの難しさは、1978年のBritainでの歯科全国調査で明らかとなった。
In the course of this survey, 720 dentate adults in Scotland agreed to permit their dental records to be followed over subsequent years.
この全国調査の過程で、Scotlandの720の歯のある成人が、複数年の歯の記録に同意した。
After 3 years, records showed that while 863 teeth in this group had been assessed as needing restorative care in the survey, 3108 actually had been restored.
調査では、本集団の863本の歯が、修復治療の必要があると評価されたが、その3年後には、3108の歯が治療を受けていた。
One might think that this finding could be explained by early lesions missed under the less-than-ideal survey conditions, but if that explanation is accepted then the next finding has no logic at all: of the 863 teeth classified as needing restorative treatment in the survey, only 271 (31%) were in the 3108 restored (Nuttall, 1983).
この発見は、理想的ではない調査状況による、初期病巣の見落としにより説明される、と考える人も、1人はいるだろう。よしんば、それで納得しても、次の発見に説明はつくのだろうか。治療を受けていた3108本のなかで、この調査で治療ニーズがあると評価された863本に含まれるのは、271本(863本の31%)[3108本の9%]なのだ (Nuttall, 1983)。
This shows that the care carried out, rather than being an extension of the survey results, in fact bore no relation to them.
これは、調査結果の延長上に、治療があるのではなく、調査結果と実際の治療には、関係がないことを示している。
This outcome is not easy to explain, but it would seem to illustrate the diverse approaches that dentists take towards diagnosing caries.
この結果を説明することは、やさしいことではないが、齲蝕の診断に対する、歯科医師のアプローチは、さまざまあることを示しているようだ。
It has been shown that dentists bring their own characteristics and biases to the task, and are largely guided by their inclinations towards particular intervention strategies.
このことから分かるのは、歯科医師は、仕事に対して自己の持ち味とバイアスをもっている、ということと、特定の介入戦略に対する性向を主な判断材料とする、ということである。
As a result, it is hardly surprising that there is substantial divergence between dentists in the nature of their diagnostic decisions (Bader & Shugars, 1997).
結果として、その性質を踏まえれば、診断は、歯科医師によって大きな隔たりがあるというのは、驚く事ではない (Bader & Shugars, 1997)。
‘Dental needs’ in the USA were assessed by examiners in the first National Health and Examination Survey (NHANES 1) of 1971-1974, and 65% of the population were judged as being in need of restorative care (US Public Health Service, NCHS, 1979).
USAにおける‘歯科ニーズ’は、1971-1974年のNHANES 1により評価され、全体の65%は、修復治療のニーズがあると判断された (US Public Health Service, NCHS, 1979)。
A similar assessment was made with the first national survey of schoolchildren in 1979/80, when 37% of schoolchildren were judged to be in need of restorative care (US Public Health Service, NIDR, 1982).
同様の評価が、1979/80年の第1回全国学童調査で行われ、学童の37%に修復治療のニーズがあると判断された (US Public Health Service, NIDR, 1982)。
These figures have received little use.
これらの数字は、ほとんど利用されていない。
In later national surveys (US Public Health Service, NIDR, 1987, 1989), treatment needs assessments were not carried out.
その後の全国調査 (US Public Health Service, NIDR, 1987, 1989) では、治療ニーズの評価は、実施されなかった。
The most recent national surveillance survey in the USA, for which data were collected during 1999-2002, reported that 16.1% of children aged 12-15 years had at least one decayed tooth (enamel or dentinal cavitation level), but the issue of ‘treatment needs’ was not brought up (Beltnin-Aguilar et al., 2005).
1999-2002年に採 取されたUSAの全国調査によると、12-15歳児の16.1%は少なくとも1つ以上の齲歯(エナメル質あるいは象牙質の齲窩)を有していたが、‘治療ニーズ’は提示されなかった (Beltnin-Aguilar et al., 2005)。[2010.2.14]
P129
The WHO includes a subjective treatment-need assessment by the examiner as part of its Pathfinder survey method (WHO, 1997), although it is not known how well these estimates approximate treatment actually carried out.
WHOは、パスファインダー調査 (WHO, 1997) の一環として、検査者による主観的な治療ニーズの評価を盛り込んだが、実際に行われた隣接面治療をどの程度見積もっているのかは、不明である。
WHO also has developed a broad-based approach to determining needs in low-income countries through what it calls a situation analysis, an enhancement of Pathfinder survey data with information on population trends, school enrollment figures, per capita income and health-care resources (WHO, 1980).
WHOは、いわゆる状況分析、集団の傾向の情報をもったパスファインダー調査の資料の強化、学校入学者の数字、一人当たりの収入と医療資源を通じて、低所得国家におけるニーズを決定するための広範なアプローチを開発している。
Distribution of caries
齲蝕の分布
Global distribution
世界的な分布
Caries has historically been seen as a disease of the high-income countries, with a low prevalence in poorer countries.
齲蝕は歴史的に、高所得国家の疾病であり、低所得国家における有病割合は低い。[2010.2.15]
The most obvious reason for this pattern is usually considered to be diet: high consumption of refined carbo-hydrates and other processed foods in the high-income countries and hunting and subsistence farming in the low-income countries.*
この傾向の最も著名な理由は、通常、食事にあると考えられている。高所得国家における精製された炭水化物と加工食品の過剰摂取、そして低所得国家における最低限の自給自足である。*
Some of the historic patterns of high attrition, little coronal caries and moderate prevalence of root caries described above, can still be found in some parts of the world, but they are fast disappearing as once-isolated populations increasingly adopt the cariogenic diets and cultural lifestyles of the high-income world.
上記した、強い磨滅とほとんどない歯冠齲蝕、中程度の有病割合の根面齲蝕という歴史的な傾向は、いまだに世界の一部で確認される。しかし、かつては孤立していた集団が、高所得世界の齲蝕原性食品と文化的生活習慣に適応していくにつれて、これらは消えてきている。
* The World Bank classifies countries as high-income, high middle-income, low middle-income and low-income.
* 世界銀行は、国家を、高所得国家、中高所得国家、中低所得国家、低所得国家に分けている。
These terms replace such words as developed/developing and industrialized/non-industrialized.
これらは、先進国、開発途上国あるいは工業国、非工業国といった言葉と置き換えされる。
See the World Bank website:
世界銀行の公式ウェブサイト:
http://www.worldbank.or.gldata/countryclass/classgroups.htm
There is good evidence that this historical pattern was clearly changing by the later years of the twentieth century.
この歴史的な傾向が、20世紀の終焉までに、疑いようもなく変化してきているという、すぐれた検証がある。
First, there was evidence that caries experience in some low-income countries had risen in the years after World War II (1939-1945) (Moller et al., 1978), although this change was by no means universal, with some populations, notably in Africa, remaining relatively unaffected (Chironga & Manji, 1989; Mosha & Robison, 1989; Manji & Fejerskov, 1990; Baelum et al., 1991; Mosha & Scheutz, 1992; Mosha et al., 1994).
第1に、この変化は、決して普遍的なものではなく、Africaなどいくつかの国では、比較的この変化が見られないのであるが (Chironga & Manji, 1989; Mosha & Robison, 1989; Manji& Fejerskov, 1990; Baelum et al., 1991; Mosha & Scheutz, 1992; Mosha et al., 1994)、低所得国家の一部では、第二次世界大戦(1939-1945年)以降、齲蝕経験が上昇してきているということである (Moller et al., 1978)。[Mollerは正しくは、Møller]
The second change is the marked reduction in caries experience among children and young adults in high income-countries, a trend that first became evident in the late 1970s (Burt, 1978).
第2に、1970年代の後半から始まった、高所得国家の小児と若年者の齲蝕経験の、目を見張る減少である (Burt, 1978)。
This change affects the oral conditions of the whole population in due course as today’s younger cohorts progress through the lifespan.
こちらの変化は、今日の若年者の加齢にともない、近いうちに、集団全体の口内状況に影響する。
WHO maintains the Global Oral Health Data Bank, a collection of surveillance data from most of the world’s countries.
WHOはGlobal Oral Health Data Bankを維持しており、世界のほとんどの国から調査資料を収集している。
As in any surveillance system where a data collection protocol is used in a multitude of different situations by different people, there are likely to be some in consistencies in these data.
どのような調査制度にでも見られるが、資料採取手順は、さまざまな人々により異なる状況により、利用されており、これらの資料には、何らかの一貫性のなさがありがちである。
Still, the data bank provides an invaluable profile of broad trends in oral health.
それでも、データバンクは口内保健のさまざまな傾向の計り知れない輪郭をもたらす。
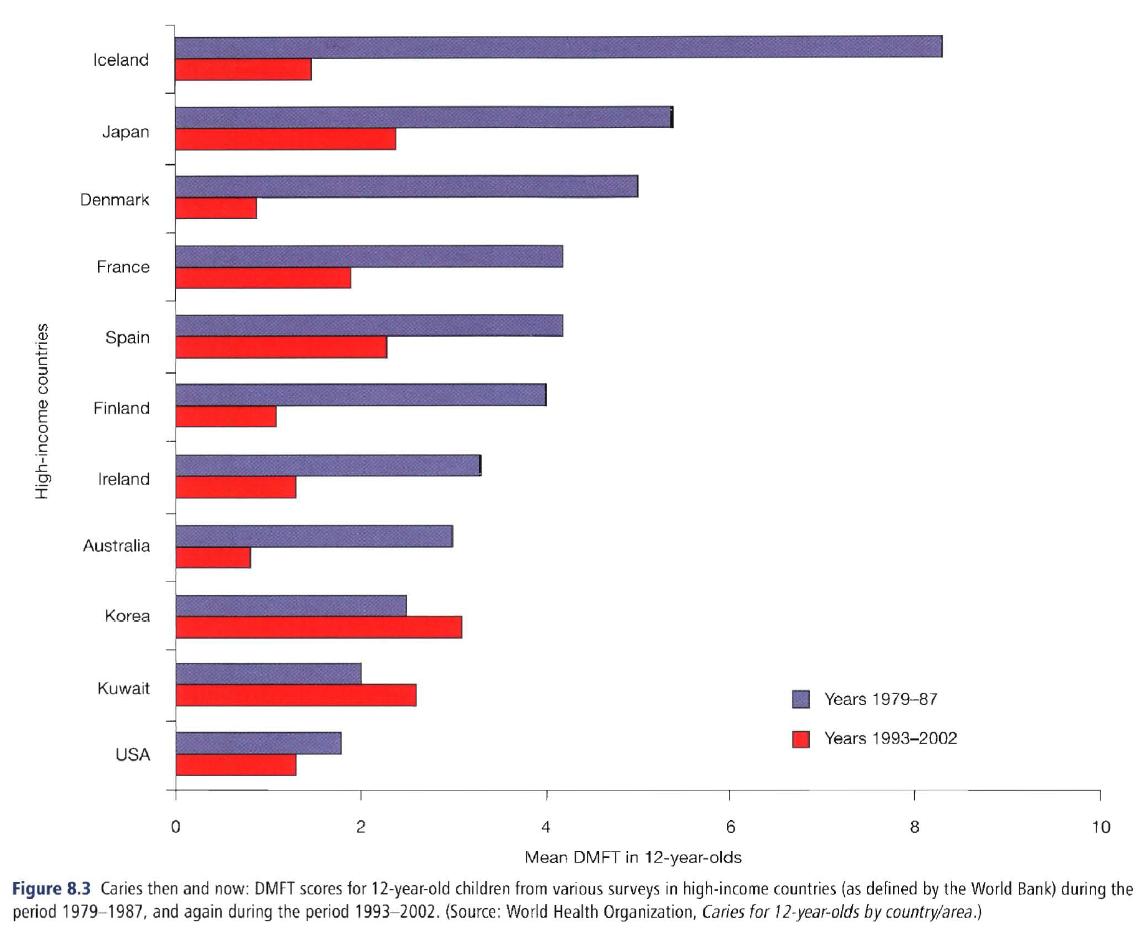 Figure 8.3 uses figures from the Global Oral Health Data Bank and from the World Bank to show the trends in DMFT scores in 11 high-income countries from 1979-1987 and from 1993-2002.
Figure 8.3 uses figures from the Global Oral Health Data Bank and from the World Bank to show the trends in DMFT scores in 11 high-income countries from 1979-1987 and from 1993-2002.
Figure 8.3は、世界銀行のGlobal Oral Health Data Bankの数字から、1979-1987年と1993-2002年の11の高所得国家におけるDMFTスコアの傾向を示している。
For most of these countries the decline in caries levels has been substantial, but again it is not universal because both Korea and Kuwait have seen a rise in DMFT scores.
これらの国のほとんどでは、齲蝕水準の大規模な減少が生じているが、やはりこれも普遍的なものではなく、KoreaとKuwaitではDMFTスコアの増加がみられる。[2010.2.16]
This could be because preventive measures have lagged behind rapidly growing affluence (and hence easier access to cariogenic diets) in these countries.
これは、これらの国での豊かさの急速な広まり(と、それによる炭水化物摂取の増加)の背後で、予防対策が遅れを取っていることにある。
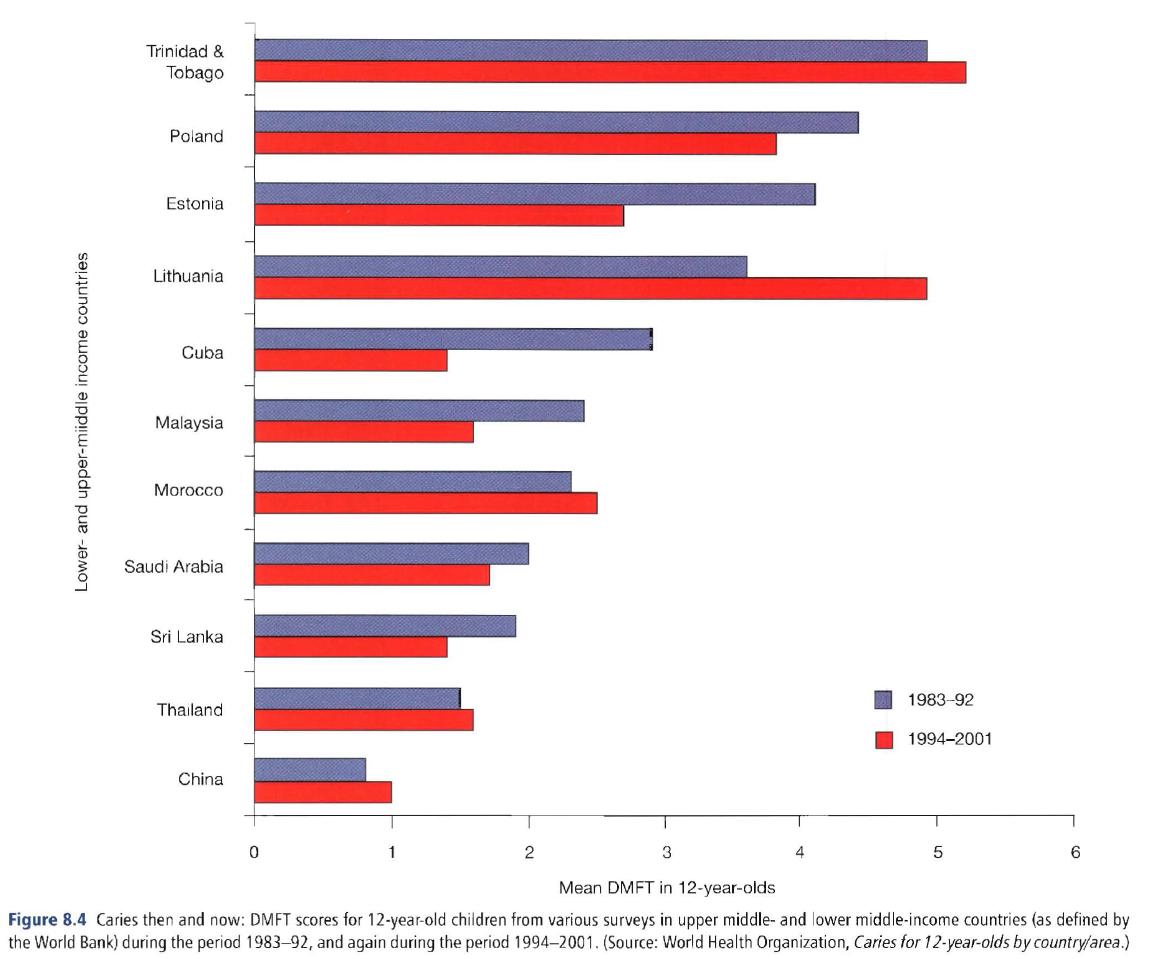 Figure 8.4 shows the same display for selected upper middle- and lower middle-income countries, those without the same resources as the countries in Fig. 8.3, and here the pattern is different.
Figure 8.4 shows the same display for selected upper middle- and lower middle-income countries, those without the same resources as the countries in Fig. 8.3, and here the pattern is different.
Figure 8.4は、中高所得国家と中低所得国家を選び、DMFTスコアをあらわしているが、傾向に違いのあることがお分かりだろうか。
Only Cuba, which has had a school dental service for years, and Estonia, where caries levels were very high, have shown a substantial drop in caries patterns over the past 20-25 years.
数年にわたり学校歯科医療を行っているCuba、そして齲蝕水準の高いEstoniaでは、この20-25年の間に、齲蝕傾向の大きな減少が見られる。[Cubaは上から5番目、Estoniaは上から3番目]
Of the others, four have shown a minor decline, and four have had an increase.
そのほかの国では、4ヶ国に、わずかな減少が、5ヶ国には上昇が認められる。
They do show a pattern: nations with better developed public health prevention programs generally have shown most success with caries reduction.
これには、ある傾向が見られる。公衆衛生予防計画が進んでいる国ほど、齲蝕減少に成功しているのである。[...prublic health prevention programs...ね][2010.2.17]
However, distinct differences in caries experience exist from one country to another and from region to region within a country.
しかし、国ごと、そして国内の地域ごとにも、齲蝕経験の格差は存在している。[2010.2.19]
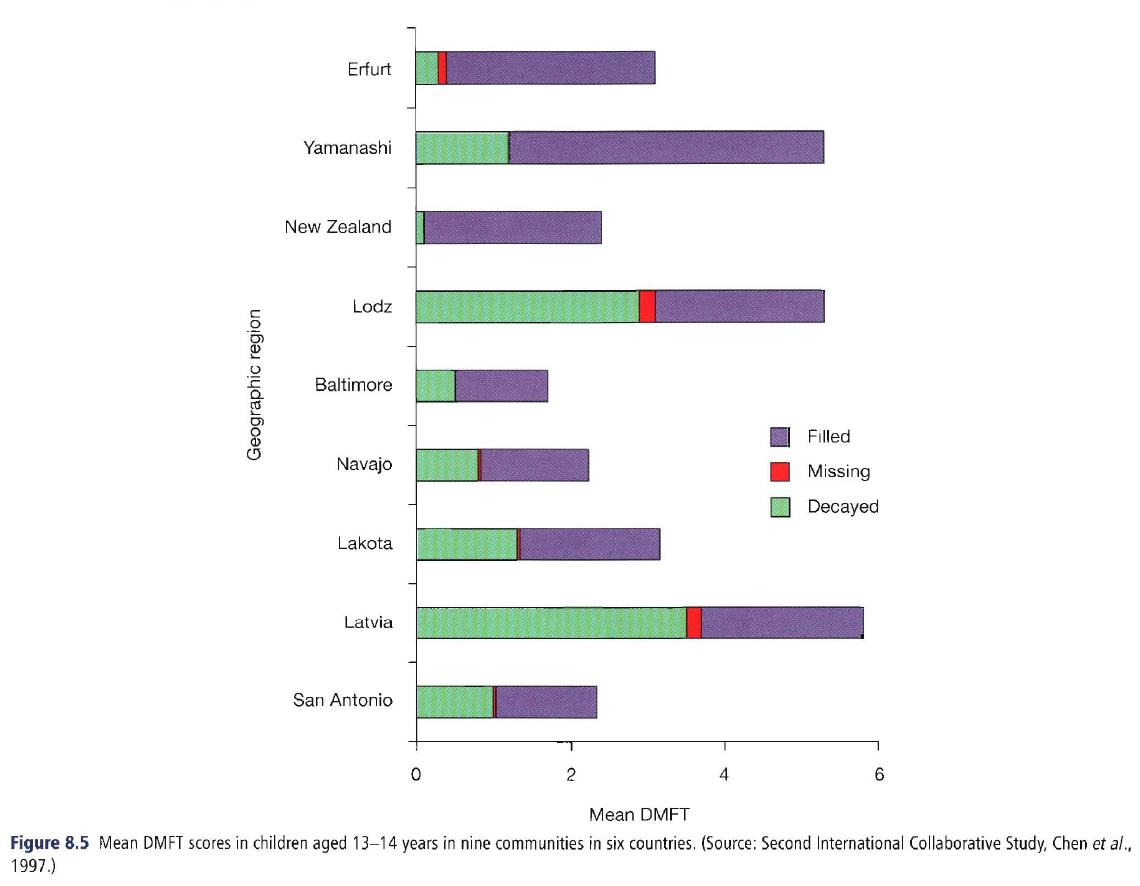 Intercountry differences are illustrated by the results of the second International Collaborative Study (ICS II) in the 1990s (Chen et al., 1997), shown in Fig. 8.5.
Intercountry differences are illustrated by the results of the second International Collaborative Study (ICS II) in the 1990s (Chen et al., 1997), shown in Fig. 8.5.
Fig. 8.5には、国内格差の実態を、1990年代の第2回国際協力研究 (ICS II) に基づき示した (Chen et al., 1997)。
The 13-14-year-old children examined were from selected communities rather than from nationally representative population samples, so there is a possibility of selection bias in these data.
診査された13-14歳児は、国を代表する標本ではなく、ある地域からの標本なので、これらの資料にはセレクションバイアスがあるかもしれない。
The highest caries levels are seen in Eastern European countries and Japan.
もっとも齲蝕水準が高いのは、東欧諸国と日本である。
Differences in caries experience between countries are not always easy to explain, but can often be seen to stem from sample selection and variable caries criteria.
齲蝕経験の国家間の格差は、簡単に説明できるわけではないが、標本抽出と齲蝕の基準のばらつきに起因するものと考えられる。
Secular variations in caries extent and severity
齲蝕の広がりと重症度の経年的ばらつき
Several reports from both national data and local surveys by the early 1980s suggested that the previously high DMF scores in high-income countries were diminishing (Hunter, 1979; McEniery & Davies, 1979; Sardo Infirri & Barmes, 1979; Hugoson et al., 1980; Anderson et al., 1981; Glass, 1981; Hughes & Rozier, 1981; Bryan et al., 1982; Fejerskovet al., 1982; Stookey et al., 1985).
1980年代初頭の全国資料と地方の調査の両方が、高所得国家のDMFスコアは、以前より低下していることを示唆していた (Hunter, 1979; McEniery & Davies, 1979; Sardo Infirri & Barmes, 1979; Hugoson et al., 1980; Anderson et al., 1981; Glass, 1981; Hughes & Rozier, 1981; Bryan et al., 1982; Fejerskovet al., 1982; Stookey et al., 1985)。
In the USA, as one example, this decline in caries prevalence and severity was confirmed by results from the National Dental Caries Prevalence Survey in US School Children of 1979/80 (US Public Health Service, NIDR, 1981).
USAでの1つの例としては、1979/80年のUS学童齲蝕有病割合全国調査の結果により、齲蝕の有病割合と重症度が低下していることが確認されている (US Public Health Service, NIDR, 1981)。
This survey found that mean DMF scores among children aged 5-17 years were some 32% lower than those in the first National Health and Nutrition Examination Survey of 1971-1974 (US Public Health Service, NCHS, 1981).
この調査は、5-17歳児の平均DMFスコアは、1971-81年のNHNES I(第1回保健栄養全国調査)よりも32%低くなったことを示していた (US Public Health Service, NCHS, 1981)。
The next national survey of US schoolchildren in 1986/87 found that the decline was continuing (US Public Health Service, NlDR, 1989), with mean DMF scores for 5-17-year-olds again 36% lower than those from seven years earlier, and this trend continued through the national survey of 1988-1994 (US Department of Health and Human Services, 1997).
1986/1987年のUS学童全国調査は、この減少傾向が継続していることを示し (US Public Health Service, NlDR, 1989)、5-17歳児の平均DMFスコアは、7年前と比較して、さらに36%低下し、この傾向は1988-1994年の全国調査でも継続していた (US Department of Health and Human Services, 1997)。
P130
The caries decline in the permanent dentition continues to the present day, and is apparent in just about all of the high-income countries.
永久歯にみられる、この齲蝕減少傾向は、今日まで継続しており、ほぼすべての高所得国家に見られている。
 As an example from the USA, Fig. 8.6 shows the average DMFT scores among children of three different age groups in the two most recent national surveys, only some 8-11 years apart.
As an example from the USA, Fig. 8.6 shows the average DMFT scores among children of three different age groups in the two most recent national surveys, only some 8-11 years apart.
このUSAの例として、Fig. 8.6は(8-11年間隔の)直近2回の全国調査における3つの年代の児童の平均DMFスコアを示す。
Another example comes from Australia, where the city of Tamworth was the site of a series of dental surveys over a period of 25 years.
Australiaから、もう1つの例がある。Tamworthの街は25年間隔で歯の調査を行っている。
The first survey was a baseline for Tamworth’s commencement of water fluoridation in 1963, and the surveys of school children continued periodically until 1988.
この調査は、水道水フッ化物添加を開始した1963年をベースラインとしており、1988年まで定期的に学童の調査を行っていた。
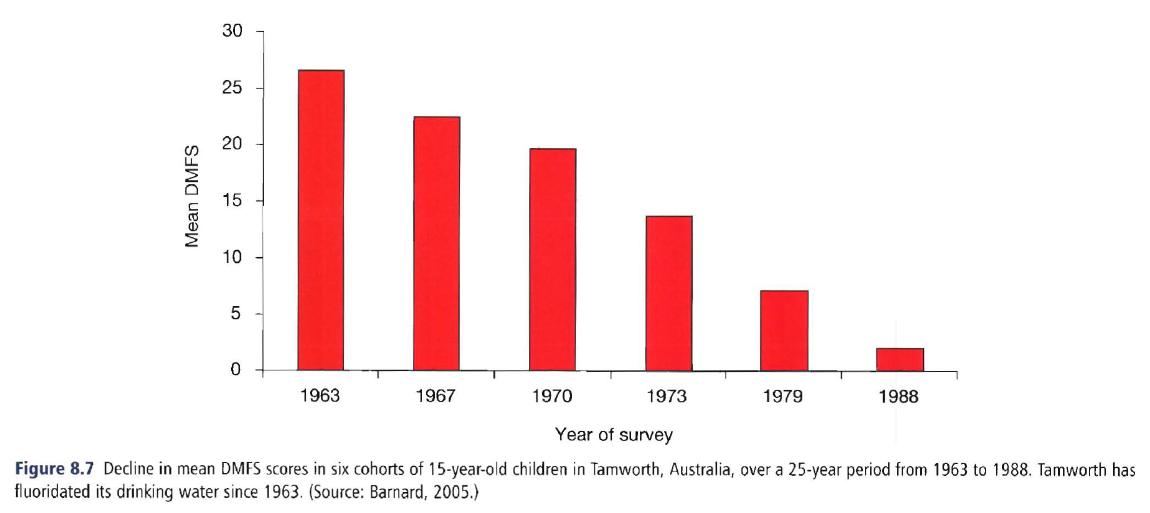 Figure 8.7, in which the data are all for 15-year-old children, shows the trend of constantly diminishing caries experience in Tamworth over a period of increasing use of fluoride.
Figure 8.7, in which the data are all for 15-year-old children, shows the trend of constantly diminishing caries experience in Tamworth over a period of increasing use of fluoride.
Figure 8.7は、15歳児の資料であり、Tamworthでは、フッ化物応用が進んだ時期に、齲蝕経験が減少し続けた傾向が示されている。
The DMF index, as described above, is a measure of average caries severity in terms of the number of teeth affected by caries.
DMF指数は、以上に示したように、齲蝕に侵された歯の数という意味で、齲蝕の平均的重症度の指標である。
Another measure, more readily understood by other health professionals and the public, is prevalence, defined as the number of disease cases at a given time (while incidence is the number of new disease cases over a specified time).
医師や一般の人々により容易に理解される指標は、有病数である。これはある1時点における疾病の数として定義される。(これに対して、発生数は、特定の期間に新たに発生した疾病の数である。)[この定義は、疫学事典によればpoint prevalenceに近い]
It is shown in Chapter 9 that caries is a process, thus making it difficult to say exactly when caries starts.
Chapter 9に示すように、齲蝕はプロセスであり、厳密に齲蝕がはじまった時点を特定するのは、容易ではない。
Chapter 9 also makes the point that there really is no such thing as ‘caries free’.
Chapter 9では、実際に‘齲蝕なし’なんぞ、ありえない、としている。
However, public health workers need to be able to identify those children who need operative or non-operative treatment, and a convenient marker for that is ‘free of obvious caries’, i.e. open cavities or tissue loss in fissures that are readily detectible.
しかし、公衆衛生担当者は、外科的治療や非外科的な治療を必要とする小児を特定する必要があり、‘明らかな齲蝕(容易に検出可能な開いた窩洞や裂溝の組織欠損)はない’というのは、その便利な指標である。[2010.2.20]
So ‘prevalence of caries’, as the term is used in public health surveillance and programming, means the proportion of a population that has at least one obvious lesion (or a restoration or extraction due to caries).
だから、‘齲蝕の有病割合’は、公衆衛生調査と計画で使われるときには、最低でも1つの明らかな病巣(あるいは、齲蝕による修復か抜歯)のある人の割合を意味する。[疫学事典でも説明されますが、proportion割合とrate率は、異なる定義が与えられていますので、区別が必要です]
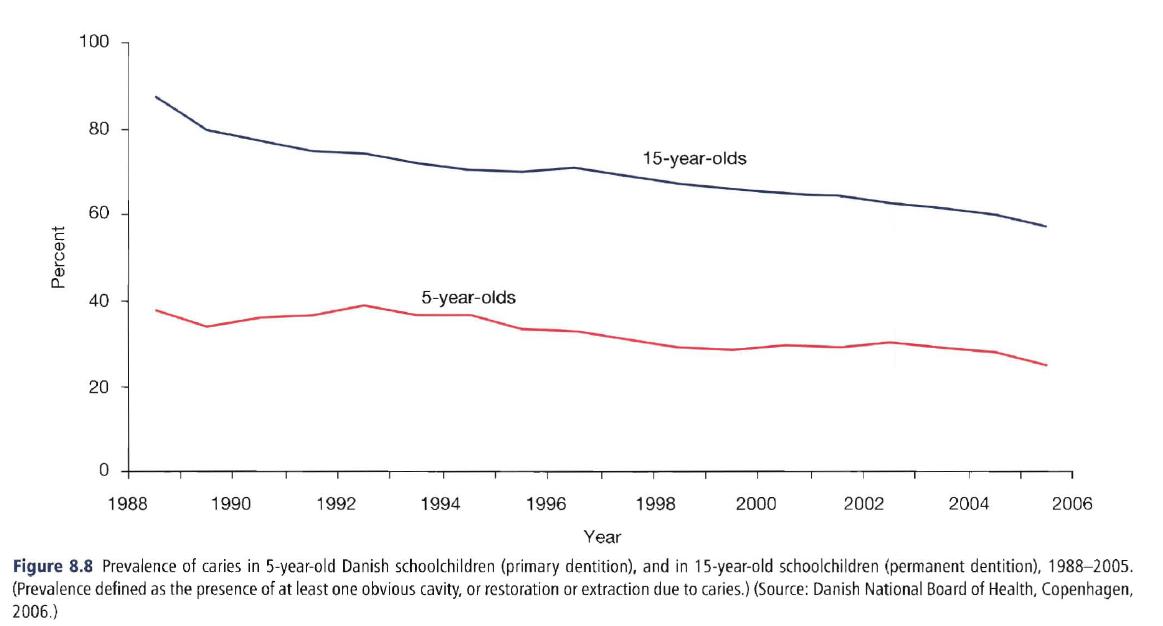 Looking at such data from the Danish School Dental Service over the period from 1988 to 2005 (Fig. 8.8), it can be seen that the prevalence of caries has dropped steadily over the years, both in the primary dentition (5-year-olds) and in the permanent dentition (15-year-olds).
Looking at such data from the Danish School Dental Service over the period from 1988 to 2005 (Fig. 8.8), it can be seen that the prevalence of caries has dropped steadily over the years, both in the primary dentition (5-year-olds) and in the permanent dentition (15-year-olds).
1988-2005年のDanish School Dental Serviceの資料 (Fig. 8.8) を見ると、乳歯(5歳児)と永久歯(15歳児)の両方で、齲蝕有病割合は年を追って低下してきている。
P131
The seemingly sudden decline in caries among children in high-income nations (which was perhaps not all that sudden because there are data to suggest that it might have started in the 1960s: Fejerskov et al., 1982; Burt, 1985) was documented at a 1982 conference in Boston, the proceedings of which were published in a special issue of the Journal of Dental Research in November 1982.
高所得国家における小児齲蝕の、一見、突然の減少(1960年代から始まっていることを示唆する資料があるので、それほど突然でもないのだが: Fejerskov et al., 1982; Burt, 1985)は、1982年11月のJournal of Detnal Researchのspecial issueで公開する過程で、同年のBoston合意会議にて明らかにされた。
The decline in caries in the permanent dentition among children of the high-income nations has continued since then (Kumar et al., 1991; Bjarnason et al., 1993; Athanassouli et al., 1994; Downer, 1994; Spencer, 1994; Marthaler et al., 1996; Truin et al., 1998; Carvalho et al., 2001).
高所得国家の小児の永久歯の齲蝕の減少は、当時から現在まで継続中である (Kumar et al., 1991; Bjarnason et al., 1993; Athanassouli et al., 1994; Downer, 1994; Spencer, 1994; Marthaler et al., 1996; Truin et al., 1998; Carvalho et al., 2001)。
The main caries problem in the high-income countries today is not so much overall caries levels, but rather the disparities in disease experience and treatment between different socioeconomic and racial/ethnic groups.
今日では、高所得国家における齲蝕は、齲蝕水準ではなく、SESや人種による、疾病経験や治療の格差が、主な課題となっている。[2010.2.21]
Regarding caries trends in the primary dentition, there is evidence that the caries decline paralleled that seen in the permanent dentition until around the late 1980s to early1990s, when the decline seemed to level out (Hargreaveset al., 1987; Brown et al., 1995; Kaste et al., 1996; Marthaleret al., 1996; Poulsen, 1996; Speechley & Johnston, 1996; Truin et al., 1998; Poulsen & Scheutz, 1999).
1980年代の終わりから1990年代初期にかけて永久歯に見られたような齲蝕の減少の停滞は、乳歯の齲蝕に関しても同様である、という検証がある (Hargreaveset al., 1987; Brown et al., 1995; Kaste et al., 1996; Marthaleret al., 1996; Poulsen, 1996; Speechley & Johnston, 1996; Truin et al., 1998; Poulsen & Scheutz, 1999)。
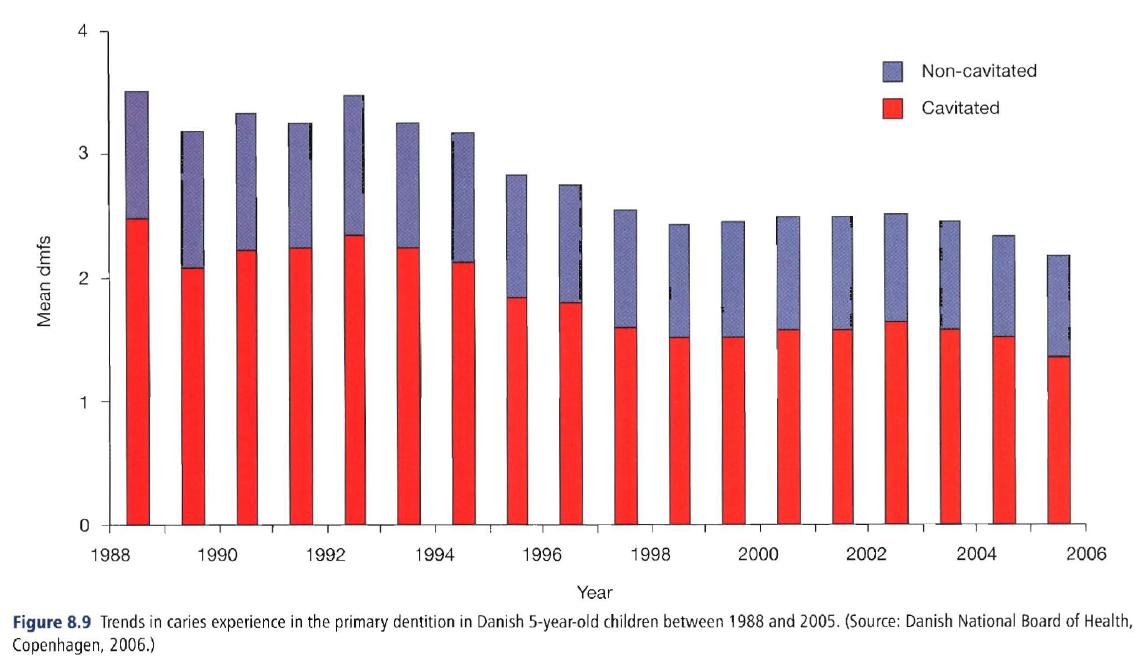 Data from the Danish School Dental Service shown in Fig. 8.9 and covering the period from 1988 to 2005, however, suggest that another decline was evident in the early 1990s, followed by a plateauing from then to the present.
Data from the Danish School Dental Service shown in Fig. 8.9 and covering the period from 1988 to 2005, however, suggest that another decline was evident in the early 1990s, followed by a plateauing from then to the present.
しかし、Figure 8.9に示した、1988-2005年を対象にしたDanish School Dental Serviceの資料は、1990年代初期の減少に続いて停滞が生じていることを示唆している。
(Figure 8.9 also demonstrates again how including or excluding non-cavitated lesions in the recording affects the outcome.)
(Figure 8.9は、記録に齲窩のない病巣を含むかどうかが結果にもたらす影響についても、示している。)
P132
P133
The reduction in caries has not occurred evenly across all kinds of tooth surfaces, for it has been proportionately greater in free smooth surfaces and proximal surfaces than in pit-and-fissure surfaces (Bohannon, 1983; Stamm, 1984).
齲蝕の減少は、あらゆる歯面に等しく生じるのではない。平滑面と隣接面に生じた減少は、小窩裂溝に生じた減少よりも大きい (Bohannon, 1983; Stamm, 1984)。
In a 3-year longitudinal study in Michigan in the early 1980s, 81% of all new lesions were on occlusal surfaces and in the pits and fissures of buccal and lingual molar surfaces, with no lesions at all on free smooth surfaces (Burt et al.,1988).
1980年代初期のMichganの3年間の縦断研究では、咬合面の新たなる齲蝕病巣の81%は、臼歯の咬合面と頬舌面の小窩裂溝に生じており、平滑面には生じていなかった (Burt et al.,1988)。[残り19%は隣接面、ということか?]
The net result is that while the total number of new carious lesions has been dropping, an increasing proportion of them is made up of pit-and-fissure lesions.
新たなる齲蝕の総数は減ったため、小窩裂溝齲蝕の割合が増えているという、結果であった。
As caries prevalence falls, the least susceptible sites (proximal and smooth surfaces) reduce by the greatest proportion, while the most susceptible sites (occlusal) reduce by the smallest proportion (McDonald & Sheiham,1992).
齲蝕有病割合は低下しているが、感受性の低い部位(隣接面と平滑面)は、齲蝕の減少が大きく、感受性の高い部位(咬合面)は、齲蝕の減少が小さい。 (McDonald & Sheiham,1992)。
History has many examples of diseases that have waxed and waned without a firm understanding of why, and caries is one of these.
歴史は、人類による確固たる理解を寄せ付けずに猛威を奮い、また衰退の途をたどる疾病のさまざまな例を見せてくれる。そして、齲蝕は、そのような疾病の1つである。
No clear reasons for the caries decline have been identified, although most researchers see the various uses of fluoride as the main reason (Bratthall et al., 1996).
齲蝕の減少の原因は明らかではないが、多くの研究者は、主たる原因は、さまざまなフッ化物応用にあると、にらんでいる。
However, fluoride alone does not explain more than about 50% of the reduction (Marthaler et al., 1996), and we still do not have a clear understanding of the relative strength of caries risk factors.
しかし、フッ化物は、齲蝕減少の50%程度を説明するに過ぎず (Marthaler et al., 1996)、私たちは、齲蝕のリスクファクターの相対的重要性については、よく理解していない。
Sugar consumption, in the USA at least, has increased rather than diminished, and there is no good evidence concerning the roles of better oral hygiene, changes in the bacterial ecology of the oral cavity and the widespread use of pediatric antibiotics on oral bacteria.
少なくともUSAでは、砂糖消費は勢いを増しており、また、口内衛生、口内細菌叢の変化、口内細菌への小児抗菌薬の広範な使用のはたらきについての検証は、ない。[2010.2.22]
Many see a likely impact, though as yet unquantified, from raised living standards that come with indoor plumbing, and elevated social norms concerning laundry, personal hygiene and grooming.
現在のところ数量化の兆しは無いが、多くの人々は、室内トイレ、洗濯ものに関する気高い社会規範、個人衛生、身繕いとともに改善された生活基準の影響とみている。[この辺はMcKeownのRole of medicineに詳しい]
Better oral hygiene can easily be seen as part of more meticulous personal hygiene and grooming rather than a conscious act to improve oral health.
口内衛生は、口内衛生の改善への意識的行為というより、行き届いた個人衛生と身繕いの一部であると思われる。[死語・廃語かもだけど、エチケット、ね]
As with the cyclical nature of other diseases over time, however, it is quite likely that there are factors operating that have not been identified (see discussion later in this chapter on the effect of the social environment).
長期的に見られるその他の疾病の循環性と同様に、齲蝕の減少は特定されていないファクターによるものなのかもしれない(社会環境の影響については本chapterの後半で論じる)。[2010.2.23]
The uneven distribution of caries
齲蝕の不公平な分布
For many years, the results of national surveys were presented only as mean DMF values, usually with only a standard deviation to indicate the distribution.
長年、全国調査の結果は、DMFスコアの平均値と標準偏差のみが公開されていた。[2010.2.24]
While means are valid and useful, they ‘compress’ extreme values, meaning those with no caries and those with a lot, into an average figure which sometimes can be misleading.
平均値は、妥当性があり便利であるが、極端な値を‘圧縮’する。つまり、齲蝕の無い人と齲蝕の多い人を、しばしば誤解をともなう、平均値に丸めてしまう。
A break from this convention in the USA came with the results of a major preventive study in the mid-1980s, which drew attention to the fact that while average caries experience in children was lower than the researchers had originally expected, there was still a significant minority with severe caries (Graves et al., 1986).
USAでは、1980年代半ばに大きな予防研究があり、その前後の全国調査の結果を検討すると、小児の齲蝕経験の平均は、研究者が当初予想していたよりも低くなったが、重度の齲蝕を抱えたままの集団も、わずかながら存在している、という事実に注意が向けられるようになった (Graves et al., 1986)。
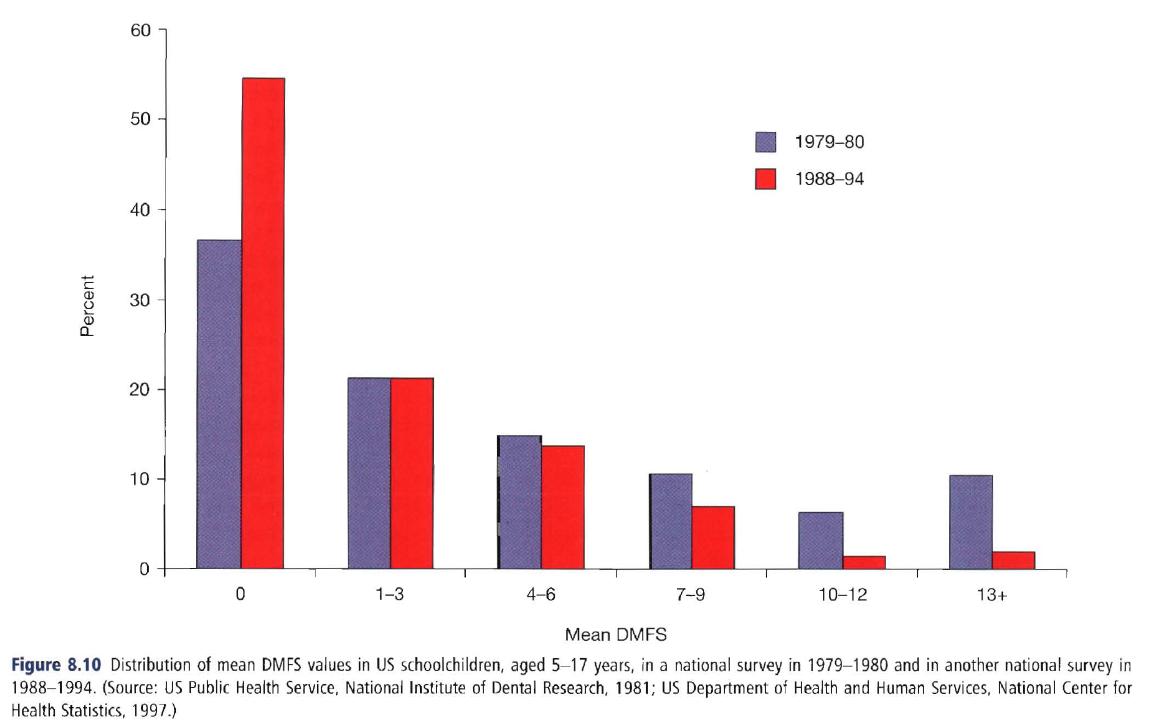 This type of distribution is illustrated in Fig. 8.10, which shows data from the US national surveys of schoolchildren in 1979-1980 and 1988-1994.
This type of distribution is illustrated in Fig. 8.10, which shows data from the US national surveys of schoolchildren in 1979-1980 and 1988-1994.
この分布の傾向をFig. 8.10に示した。1979-1980年と1988-1994年のUS学童全国調査の資料である。
Rather than mean DMF scores, this graph illustrates the distributional changes and shows a classic skewed distribution.
このグラフは、DMFスコアの平均値ではなく、分布の変化と古典的な傾斜分布を示している。
It is evident that in the more recent survey the proportion of children with low DMF scores had increased, while the proportion with high scores (i.e. severe caries) had decreased.
最近の調査では、DMFスコアの低い小児の割合が増えており、スコアの高い(重症な)小児の割合は減少している。
Even so, the shape of the distribution remained much the same: highly skewed toward zero or few DMFS teeth, but with a persistent ‘tail’, meaning children at the severe end of the scale.
そうであっても、分布の形はおおむね変わりない。DMFS歯スコア0近辺に大きな山があり、また重症を意味する分布の端に‘裾野’が伸びている。[中央値ないし最頻値が左に移動している、ってことね]
It is these children in the tails who are considered to be at high risk, and who thus absorb a lot of attention from public health services.
ハイリスクにあると考えられる小児は、この裾野の部分に存在しており、公衆衛生上の注意を引いている。
It is generally accepted today that in any population some 60-70% of all carious lesions are found in 15-25% of the children.
今日では一般に、どのような集団でも、小児の15-25%に全ての齲蝕の60-70%ほどが集中している。
Whether these children should be targeted for special preventive treatment or not remains a subject for active debate (see Chapters 28 and 29).
これらの小児を、特別な予防処置の対象とすべきかど齲窩は、活発な議論を呼んでいる(Chapter 28と29をみよ)。
Age and gender
年齢と性別
Mean DMF scores increase with age.
DMFスコアの平均値は、加齢とともに増加する。
Caries used to be considered just a childhood disease, a perception from those days of high caries severity when most susceptible surfaces were usually affected by adolescence.
青年期までに、最も感受性のある歯面が侵されていた頃、齲蝕は、幼児期の疾病であり、この時期から齲蝕は重症化すると認識されていた。
With younger people now reaching adulthood with many surfaces free of caries, the carious attack is spread out more throughout life.
現在、より若い人々は、多くの歯面に齲蝕のないまま成人しており、齲蝕の攻撃は、より人生を通じて広がっている。
Adults of all ages can, and do, develop new coronal lesions (Hand et al., 1988; Drake et al., 1994; Luan et al., 2000), and caries has to be viewed as a lifetime disease.
成人以降も、新たなる歯冠齲蝕は生涯にわたり進行しており (Hand et al., 1988; Drake et al., 1994; Luan et al., 2000)、齲蝕は一生涯の疾病であると見るべきである。
Even the skewed disease distribution seen in youth can be seen among the elderly (McGuire et al., 1993).
青年にみられる疾病の傾斜分布は、高齢者にもみられる (McGuire et al., 1993)。
In populations where caries experience is severe the disease starts early in life and is common in the young.
齲蝕経験が重い集団では、疾病は人生の早期から始まり、青年で蔓延する。
A more even occurrence of new lesions throughout life is characteristic of a lower community attack rate.
齲蝕水準の低い地域ほど、新たなる齲蝕は、[幼児期に集中するのではなく]人生を通じて均等に発生している。[2010.2.25]
Regarding gender, women usually have higher DMF scores than do men of the same age, although this finding is not universal.
性別の点で、女性は一般に同世代の男性よりDMFスコアが高いが、これは普遍的に見いだされることではない。[以下、Root cariesの後半より移動]
When observed in children, the difference has been attributed to the earlier eruption of teeth in girls, but this explanation is hard to support when the differences are seen in older age groups.
小児の男女の違いは、少女の歯の萌出の早いことに因っているが、その後の世代に表れている違いを見ると、この説明を支援することは難しい。
In those instances a treatment factor is more likely because in national survey data men usually have more untreated decayed surfaces than women, while women have more restored teeth.
後の世代を見てみると、全国調査では、一般に男性は女性より未治療の歯面が多く、女性は修復歯の数が多いため、治療ファクターがあるのかもしれない。
Women visit the dentist more frequently, so this observation is perhaps to be expected.
女性は男性よりも、頻繁に歯科を受診するので、これは、予想されることである。
In a national survey in the USA, girls aged 12-17 years had the same mean number of decayed and missing surfaces as their male counterparts, but 25% more filled surfaces (Kaste et al., 1996).
USAの全国調査によると、12-17歳の少女は、齲蝕歯面と喪失歯の平均値では少年と変わらないものの、修復歯面は25%上回っている (Kaste et al., 1996)。
One cannot conclude from these figures that women are more susceptible to caries than are men; a combination of earlier tooth eruption plus a treatment factor is a more likely explanation for the observed differences.
これらの数字から、女性は男性より齲蝕になりやすいと結論できる人は、いない。歯の萌出時期に治療ファクターを上乗せすれば、男女の違いを説明できそうだ。
P135
Root caries
歯根齲蝕
One important offshoot of the age-caries relationship is root caries, defined as caries that begins on cemental root surfaces exposed to the oral environment, and hence when bacterial plaque can accumulate around these exposed roots.
年齢齲蝕関係で忘れてはいけないのは、歯根齲蝕である。これは、口内環境に露出した歯根セメント質に生じる齲蝕で、それゆえ、露出した歯根周囲に細菌プラークが堆積すると生じる。
As mentioned above, root caries has been with humankind since our earliest days.
上記のとおり、歯根齲蝕は有史以来、人類に生じている。
Even so, awareness of root caries in the high-income countries only grew around the early 1980s with the realization that older adults were keeping more teeth than they used to.
とはいえ、高所得国家における歯根齲蝕が興隆を始めたのは、高齢者の残存歯がかつてより増えてきた、1980年代である。
Root caries is highly prevalent among older people in high-income countries (Salonen et al., 1989; Beck, 1993; Lo & Schwarz, 1994; Hawkins et al., 1998; Gilbert et al., 2001; Chalmers et al., 2002; Morse et al., 2002), although it too has declined in recent years, just as coronal caries has.
歯根齲蝕は、高所得国家の高齢者に蔓延している (Salonen et al., 1989; Beck, 1993; Lo & Schwarz, 1994; Hawkins et al., 1998; Gilbert et al., 2001; Chalmers et al., 2002; Morse et al., 2002) が、近年は歯冠齲蝕と歩みを合わせるように、減少してきている。
 Figure 8.11 shows the decline in root lesions in the USA, despite greater tooth retention, between the two most recent national surveillance surveys.
Figure 8.11 shows the decline in root lesions in the USA, despite greater tooth retention, between the two most recent national surveillance surveys.
USAでは、直近2回の全国調査の間に、より多くの歯が残るようになってきているにもかかわらず、歯根病巣は減少してきている様子が、Figure 8.11に示されている。
Root caries, by definition, is strongly associated with the loss of periodontal attachment (Locker & Leake, 1993; Slade et al., 1993; Whelton et al., 1993; Lawrence et al., 1995; Ringelberg et al., 1996).
歯根齲蝕は、本質的に、歯周アタッチメントの喪失と、強固な関係がある (Locker & Leake, 1993; Slade et al., 1993; Whelton et al., 1993; Lawrence et al., 1995; Ringelberg et al., 1996)。
Other correlates associated with root caries are primarily socioeconomic: years of education, number of remaining teeth, use of dental services, oral hygiene levels and preventive behavior (Vehkalahti &Paunio, 1988; DePaola et al., 1989; Beck, 1993;).
そのほかの歯根齲蝕と関係のあるものには、学歴[いわゆるempowerment]、残存歯数、歯科医療の利用、口内衛生水準、予防行動がある (Vehkalahti &Paunio, 1988; DePaola et al., 1989; Beck, 1993;)。
Another important risk factor is the use of multiple medications among the elderly (Kitamura et al., 1986), a common practice in institutions, and one that can promote xerostomia.
そのほかの重要なリスクファクターは、高齢者の施設での慣行であり、また口内乾燥症を促進する多剤服用である (Kitamura et al., 1986)。
Xerostomia has long been known as a major risk factor for caries among people of any age, and is particularly prevalent among those who have received radiation treatment for cancer.
口内乾燥症は、あらゆる世代にとって齲蝕の大きなリスクファクターであるとして知られているところであり、がんの放射線治療を受けた人には、特に蔓延している。
Other risk factors identified in a representative British sample of people aged 65 or more were poor oral hygiene, wearing partial dentures, sucking candies in a dry mouth and living in an institution (Steele etal., 2001).
Britishの65歳以上の人々の代表標本からわかったそのほかのリスクファクターは、不良な口内衛生、傷んだ部分床義歯、口内乾燥によるキャンディーの吸啜、施設での生活であった (Steele etal., 2001)。
Root caries is less prevalent in high-fluoride areas than in low fluoride communities (Burt et al., 1986; Stamm et al., 1990), smokers exhibit more root caries than non-smokers, and prevalence tends to be inversely related to the number of teeth remaining (Beck, 1993; Locker & Leake, 1993).
歯根齲蝕は、低フッ化物地域より高フッ化物地域で、鳴りを沈め (Burt et al., 1986; Stamm et al., 1990)、非喫煙者より喫煙に多く、残存歯数に反比例して多くなる傾向がある (Beck, 1993; Locker & Leake, 1993)。[2010.3.2]
Root caries seems to be a particular problem among older people of lower socioeconomic status, those who have lost some teeth, who do not maintain good oral hygiene and do not visit the dentist regularly.
歯根齲蝕は、社会経済的地位の低い高齢者、何本か歯の無い人、良好な口内衛生を維持しない人、定期的にしか受診をしない人には、とりわけ課題となる。
Because of our aging populations and increasing retention of teeth, it could be that the dimensions of the root caries problem will continue growing in the years ahead.
加齢と残存歯数の向上のため、歯根齲蝕は、あと何年かは繁栄し続けるだろう。
However, the decline shown in Fig. 8.11 adds strength to the argument that root caries, while not exactly going away, will continue to diminish in the population.
しかしFig. 8.11に示した減少は、歯根齲蝕は、絶滅とはいかなくとも衰退し続けるという反論を支持する。[以下、Age and genderに移動]
P136
Race and ethnicity
人種と少数民族
Global variations in caries experience result from environmental rather than from inherent racial attributes.
齲蝕経験の世界的なばらつきは、人種によるものではなく、環境によるものである。
To illustrate that point, there is evidence that some racial groups, once thought to be resistant to caries, quickly developed the disease when they migrated to areas with different cultural and dietary patterns (Beal, 1973; Russell, 1966).
このことを示すため、さまざまな文化的食事傾向が混在する地域への移住により、当時齲蝕に耐性があると考えられていた人種が、さくっと齲蝕にかかってしまう、ということが検証された (Beal, 1973; Russell, 1966)。
In the United States, to choose one example of a multiracial and multiethnic society, most surveys before the 1970s found that whites had higher DMF scores than African-Americans, although the latter usually had more decayed teeth.
USでは、多民族社会の例を選ぶために、1970年代のほとんどの調査は、白人はアフリカ系アメリカ人よりもDMFスコアが大きいことを、明らかにしていたが、アフリカ系アメリカ人は、通常齲歯をより多く有していた。
One of the early national surveys in 1960-1962 showed that whites had higher DMF scores than did African-American adults of the same age group, a difference that remained even when the groups were standardized for income and education (US Public Health Service, NCHS, 1967).
1960-1962年の全国調査の1つは、同世代の成人を比較すると、白人はアフリカ系アメリカ人よりDMFスコアが大きいことを示しており、これは、収入と教育で標準化しても、変わりがなかった (US Public Health Service, NCHS, 1967)。
This difference was still evident in a national survey from the1970s (US Public Health Service, NCHS, 1981).
この差は、1970年代の全国調査でも確認された (US Public Health Service, NCHS, 1981)。
By the time of the 1988-1994 national survey, however, there was little difference in total DMF scores between whites and African-Americans, although whites still had a higher filled component and lower scores for decayed and missing surfaces.
しかし、1988-1994年の全国調査までに、白人とアフリカ系アメリカ人のDMFスコアの違いはほとんどなくなり、また白人のF値が高くなり、DとMのスコアは低くなった。
DMF values for Mexican-Americans were in between.
メキシコ系アメリカ人のDMFスコアは、その中間である。
This turn around probably reflects improving access to care for African-Americans, although it still reflects socio-economic and cultural contrasts between the groups.
この変節は、おそらく、アフリカ系アメリカ人の医療へのアクセスの改善を反映しているが、しかし、まだ集団間の社会経済的文化的なコントラストを反映している。
Even though overall caries experience in the permanent dentition continues to decline in the USA, disparities between racial and ethnic groups in the prevalence and severity of dental caries still remain in the twenty-first century (Beltnln-Aguilar et al., 2005).
USAでは、永久歯の齲蝕経験は減少し続けているが、齲蝕の広がりと重症度の人種間格差と少数民族間格差は、21世紀においても残っている (Beltnln-Aguilar et al., 2005)。
However, the overall pattern is that there is no evidence to support inherent differences in caries susceptibility between racial and ethnic groups.
しかし、人種と少数民族により、齲蝕感受性に違いがあるという検証はない。
Far more important are socioeconomic differences and contrasting social environments, meaning differences in education, available income and access to health care.
より重要なのは、社会経済的な違いと対照的な社会環境、つまり教育の違い、所得の違い、医療へのアクセスの違いにある。[へ?医療へのアクセスの違いが、齲蝕感受性に影響するって?]
More difficult to measure are long-held cultural beliefs that affect values and behavior related to dental health.
歯科保健に対する価値と行動に影響をもたらす、長年の文化的考え方を評価することは、難しい。
However, no one doubts that these factors are present and influencing caries incidence.
しかし、これらのファクターが存在し、また齲蝕の発生に影響していることを疑うような[鈍い]人は、いないだろう。
Familial and genetic patterns
家族傾向と遺伝傾向
Familial tendencies (‘bad teeth run in families’) are seen by many dentists and have been recorded (Klein & Palmer, 1938; Klein &Shimizu, 1945; Ringelberg et al., 1974).
家族傾向(‘悪い歯は家族を駆け巡る’)は、多くの歯科医師が遭遇するところであり、記録にも事欠かない (Klein & Palmer, 1938; Klein &Shimizu, 1945; Ringelberg et al., 1974)。
However, these studies have not identified whether such tendencies have a true genetic basis, or whether they stem from bacterial transmission or continuing familial dietary or behavioral traits.
しかし、これらの研究は、この傾向が遺伝に基づくのかどうか、あるいは細菌感染によるものなのか、はたまた家族の食性や行動習慣によるものなのかを特定していない
Husband-wife similarities clearly have no genetic origin, and intrafamlial transmission of cariogenic flora, especially from mother to infant, is considered by some to be a primary way for cariogenic bacteria to become established in children (Kohler et al., 1983; Caufield et al., 2000).
夫婦が似ていることは、明らかに遺伝的な原因ではなく、齲蝕原性細菌叢の家族内感染、とりわけ母子感染は齲蝕原性細菌が小児に伝播する第一の原因であると考えられている (Kohler et al., 1983; Caufield et al., 2000)。
The lack of a demonstrable genetic influence by race, discussed above, weakens the case for genetic inheritance of susceptibility or resistance to caries, although it is interesting that Klein, years ago, concluded that the similarities within families involved ‘strong familial vectors which very likely have a genetic basis, perhaps sex-linked’ (Klein, 1946).
上に論じたように、人種による遺伝的影響は明らかではないため、齲蝕への感受性や耐性の遺伝的継承の言い分は弱いのだが、Kleinが、家族間の類似性には、‘遺伝的、おそらく伴性の、強力な家族的媒介’が関与している、と結論したことは、興味深い (Klein, 1946)。
With the explosion of research discoveries of genetic influences in many diseases, dental caries is being looked at in a different light.
多くの疾病で遺伝の影響の発見が相次いでおり、齲蝕は、違った角度から見られている。
It is plausible that host attributes that could affect an individual’s caries experience, such as salivary flow and composition, tooth morphology and arch width, are genetically determined, and the genetics of the cariogenic bacteria themselves may have an effect.
唾液流量と構成、歯の形態、歯列弓の幅といった、個人の齲蝕経験に影響を与える宿主属性は、遺伝的に決定されており、齲蝕原性細菌の遺伝は、その影響を受ける、という言説は、はもっともらしい。
However, the ready preventability of caries, indicated by the caries decline, strongly counters (if not refutes) the idea of any genetic component worth mentioning.
しかし、齲蝕が予防できることは、齲蝕の減少により示唆されているが、(もし論破されなければ)遺伝的要素に言及する価値があるという概念に対する強力な反論となる。
At present, no genetic role in caries experience has been demonstrated.
現在のところ、齲蝕経験における遺伝の役割は明らかではない。
P137
Socioeconomic status
社会経済的地位
Socioeconomic status (SES), or social class, is intended to be a broad summary of an individual’s attitudes, values and behavior as determined by such factors as education, income, occupation or place of residence.
社会経済的地位 (SES)、あるいは社会階層は、教育、所得、職業、あるいは居住地区といったファクターにより決定される個人の姿勢、価値観、行動を要約することを目的としている。
[2010.3.2]
Attitudes toward health are often part of the set of values that follow from an individual’s social standing in the community, and can help to explain some of the observed variance in health measures.
健康に対する態度は、しばしば、地域における個人の社会的立場から生じる価値観群の一部であり、また健康評価において観察されるばらつきの一部を説明するのに役立つ。
Obtaining a valid measure of SES, however, is always a problem because of the construct’s complexity.
しかし、SESの妥当な尺度を得るには、つねに、 構成の複雑さゆえの課題をはらむ。
The most commonly used measures are income and years of formal education, despite acknowledged shortcomings with the latter measure (Hadden, 1996).
最も普及している尺度は、所得と、欠点があるにもかからわず、とされる教育年数[学歴]である (Hadden, 1996)。
SES is used in research as an attribute specific to the individual, rather than to the community.
研究では、SESは、地域ではなく個人の属性として、利用される。
It is usually inversely related to the occurrence of many diseases, and to characteristics thought to affect health (Marmot & Wilkinson, 1999).
SESは、一般に、多くの疾病の発生に、また健康にに影響を与えると考えられる特性に反比例している (Marmot & Wilkinson, 1999)。
The reasons for disparities in health status between various SES strata can often seem obvious, but that is not always the case (Link & Phelan, 1996).
さまざまなSES階層間の健康状況の格差の理由は、明らかであるが、つねに真実というわけではない (Link & Phelan, 1996)。[2010.3.3]
For example, higher infant mortality in lower SES strata can be partly explained by the facts that higher SES women have easier access to prenatal care, can better afford such care, and have more time to obtain it, a deeper educational base to permit better understanding of the condition and probably less fatalistic attitudes, and perhaps some other factors.
例えば、SES階層が低いほど乳児死亡率は高いことは、SESの高い女性ほどは、妊婦管理へのアクセスがよく、管理を受ける余裕があり、妊婦管理に多くの時間を割きやすいという事実、そして、より優れた体調の理解をもたらす深い教育的素養と、おそらくは希薄な運命論的態度、その他もろもろのファクターにより、部分的に説明されうる。
However, even after all these likely variables have been factored into explaining the differences, there is still a considerable gap which defies explanation (Fuchs, 1974).
しかし、これらのありえそうな変量の全てを、格差の説明にあてても、なお説明できない大きな格差が存在している (Fuchs, 1974)。
Measurements used in science cannot always pick up all the subtleties embedded in SES.
通常、科学で利用される尺度は、SESに滲みこんでいるニュアンスを汲み取ることはできない。
These subtleties have also been seen in dental health.
これらのニュアンスは、歯科保健についても、同様である。
In one Finnish study, for instance, differences in caries experience between children in the higher and lower social classes still remained after accounting for the reported frequency of tooth brushing, consumption of sugars and ingestion of fluoride tablets (Milen, 1987).
たとえば、Finlandの研究では、高い社会階層と低い社会階層の小児の齲蝕経験の違いは、報告されているブラッシング、砂糖の摂取、フッ化物タブレットの摂取の頻度を考慮しても、なお、残っている (Milen, 1987)。[2010.3.4]
These are all individual behaviors that would be more common in higher SES strata.
これらは、すべて高いSES階層には一般的な個人行動である。
Another instance comes from Sweden, where even with the extensive Swedish welfare system a social gradient in oral health is still evident (Flinck et al., 1999; Kallestal &Wall, 2002).
Swedenの例では、手厚いSwedishの福祉制度のもとでさえ、口内保健の社会的勾配は残っているという検証がある (Flinck et al., 1999; Kallestal &Wall, 2002)。[2010.3.7]
As part of his landmark research in caries epidemiology during the 1930s and 1940s, Klein observed that overall DMF values did not vary much between SES groups, but aspects of treatment certainly did (Klein & Palmer, 1940).
Kleinは、1930年代と1940年代の齲蝕疫学の画期的な研究の一部として、DMF値そのものはSES集団間で大きくは変化しないが、治療の面では変化するということを、示した (Klein & Palmer, 1940)。
Lower SES groups had higher values for D and M, lower for F.
低いSES集団は、D値とM値が高く、F値は低い。
In the first national survey of US children in 1963-1965, white children in the higher SES strata actually had higher DMF scores than did white children in the lower strata, but African-American children showed the opposite profile (US Public Health Service, NCHS, 1971).
1963-1965年の第1回US小児全国調査では、社会階層の高い白人の小児は、社会階層の低い白人の小児よりも DMFスコアが高かったが、アフリカ系アメリカ人の小児は反対の特徴を示した。
In the white children, the F component ballooned so much with increasing SES that it lifted the whole DMF index.
白人の小児では、SESが上がるにつれてF要素がふくれあがり、F要素はDMF指数全体を引き上げる。
By contrast, the F component in the African-American children did not change with SES, with the net result that their DMF scores diminished with increasing SES.
対照的に、アメリカ系アフリカ人の小児のF要素は、SESにより変化せず、その結果、DMFスコアはSESが上がるにつれて小さくなる。
As mentioned earlier, these results from 1963-1965 showed that a ‘treatment effect’ was artificially inflating the DMF data in the white children.
先に指摘したように、1963-1965年の結果は、‘治療効果’が白人小児のDMFを人工的に膨らませているということを示している。
In today’s lower overall caries experience, however, the position has been reversed.
今日、齲蝕経験全体は小さくなってきているが、この状況に変わりはない。
During the period when the caries decline was first recognized, it was soon found that the higher SES groups enjoyed the sharpest decline in caries experience (Graves et al., 1986), so that the DMF values of children in higher SES strata are now generally well below those of children in lower SES strata.
当初、齲蝕の減少が認識された時代に、SESの高い集団は、齲蝕経験の減少が急激であったため (Graves et al., 1986)、現在は通常、SESの高い小児のDMF値は、SESの低い小児のDMF値よりも小さい。
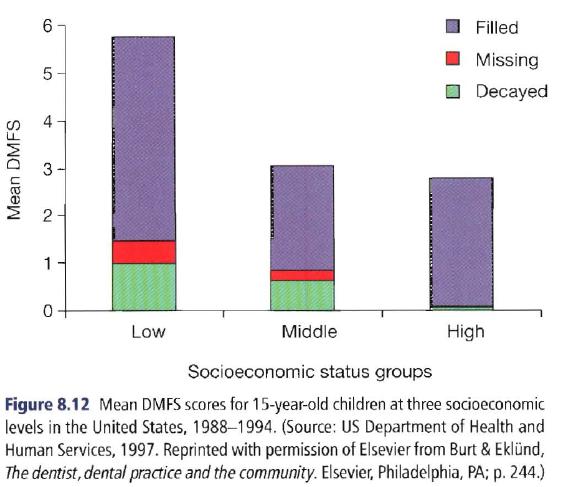 This is illustrated in Fig. 8.12, which shows the components of the DMFS index for 15-year-old children in low, medium and high SES groups from a national survey in the USA during 1988-1994.
This is illustrated in Fig. 8.12, which shows the components of the DMFS index for 15-year-old children in low, medium and high SES groups from a national survey in the USA during 1988-1994.
Fig 8.12は、1988-1994年のUSAの全国調査から、SESの低・中・高で分けた15歳児のDMFS指数の各要素を示している。
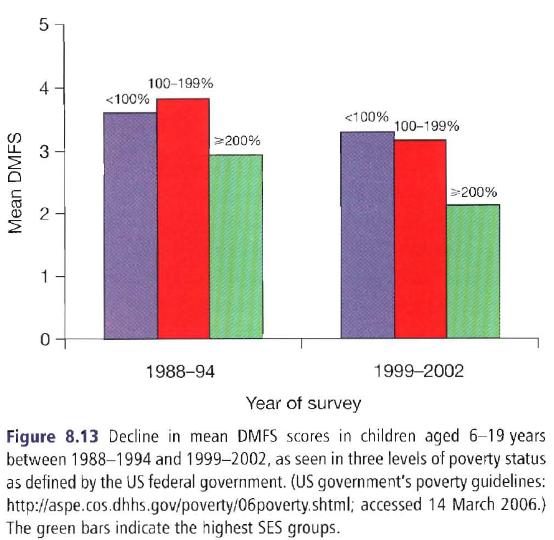 Figure 8.13 illustrates two features of the caries decline.
Figure 8.13 illustrates two features of the caries decline.
Figure 8.13は、齲蝕減少の2つの特徴を示している。[2010.3.8]
The first, the secular decline in caries, has already been illustrated (Figs 8.6-8.10) and is seen again with the reductions over time in each poverty-status group in Fig. 8.13, showing that, even over this fairly short period of 8-11 years, caries levels across all age and socioeconomic groups have continued to decline.
第1に、齲蝕の減少は、すでに示した通り (Figs 8.6-8.10) であるが、Fig 8.13に示された貧困な状況の集団のそれぞれにおいても、長期にわたる減少がみられ、8-11年というかなり短い期間に、あらゆる世代、社会経済的集団において齲蝕水準は減少し続けていることを示している。
The second aspect illustrated here is how caries levels are related to SES.
第2に、ここに示されているのは、齲蝕水準がどの程度SESに関連しているのか、ということである。
The children are grouped by poverty status as defined by the US federal government (a socioeconomic measure used to determine eligibility for government programs), and it can be seen that children in the higher SES groups (i.e. those at ≥200% of the poverty level) have lower caries scores than do children below the poverty level or only just above it.
小児は、US連邦政府により定義されている貧困状況(政府計画の資格を決定するために利用される社会経済的評価)によって分類され、Fig 8.13はSESの高い集団(貧困水準の200%以上に位置する集団)の小児は齲蝕スコアが、貧困水準あるいは、それより上の小児より低いことを示している。
P138
As noted above, it is difficult for any one measure to capture all the nuances of SES.
上記の通り、どのような評価であれ、SESのあらゆるニュアンスを汲み取ることは、難しい。
British studies have explored the issue by introducing broader measures of SES determinants, such as private housing and car ownership, that go beyond just education and income (Palmer & Pitter, 1988; Carmichael et al., 1989; Gratrix & Holloway, 1994).
Britishの研究は、教育と所得のみならず、私邸、自家用車の所有といった、SESの決定要因の広範な評価を導入し、齲蝕との関係を探索した (Palmer & Pitter, 1988; Carmichael et al., 1989; Gratrix & Holloway, 1994)。
These measures were all related to caries levels in the population.
これらの評価は、すべて、集団の齲蝕水準に関係していた。[これ、単なる交絡のような]
A better sense of coherence among poor parents of adolescent children, i.e. people who have a more structured life than do others in the same social circumstances, is related to lower caries levels among their children (Freire et al., 2002).
青年期の人々においては、両親の首尾一貫感覚が優れている(例えば、同じ社会環境で、他の人よりも、構造化された生活を送る)ことと、齲蝕水準が低いことは、関連している (Freire et al., 2002)。[sense of coherenceは首尾一貫感覚。self-efficacy自己効力感に似た概念か?][poor parentsのpoorは誤植か?]
This is an intriguing area for further research.
これは、将来の研究において、興味をくすぐる分野である。
Caries levels are also related to the degree of neighborhood deprivation, where several area summary measures have been used (Jones et al., 1997a; Jones & Worthington, 1999; Grayet al., 2000).
齲蝕水準は、近隣地域の剥奪程度に関連しており、いくつかの地域の要約指標が使われている (Jones et al., 1997a; Jones & Worthington, 1999; Grayet al., 2000)。
These broad measures of area deprivation lead directly into the role of social determinants.
これらの貧困地域の広範な評価は、直接、社会的決定要因の役割に直結している。
Caries and the social environment
齲蝕と社会環境
A useful definition of public health is ‘ ... assuring conditions in which people can be healthy’ (JOM, 1988) (with emphasis on the word can).
公衆衛生の便利な定義は、‘人々が健康に生活できる状況の保証’である(できるという表現に注目せよ) (JOM, 1988)。[though the organized effort of societyが入っていないと、どうもしっくりしませんが]
That covers everything from maintaining the stratospheric ozone layer to picking up the garbage, to providing recreational facilities, decent housing or dental care where needed.
公衆衛生は、成層圏のオゾン層を維持することから、ごみ拾い、娯楽施設やちゃんとした住居、必要とされる場所での歯科医療の提供まで、あらゆる活動にまたがる。[to pickingとto providingの接続詞が無いような]
While it stresses the public responsibility for a healthy physical and social environment, it still leaves room for individuals to exercise personal choice in their health-related behavior and how they use health-care services.
公衆衛生は、健康的な物理的社会的環境に対する公的責任を強調するが、個人が、保健関連行動と医療をどのように利用するかという個人的選択を行使する余地を残している。[2010.3.10]
The term social determinants is related to this definition in that it refers to factors that affect health outcomes for everyone in the community, and whose presence or absence influences the environment ‘in which people can be healthy’.
社会的決定要因という言葉は、地域に住むすべての人のヘルスアウトカムに影響を与えるファクターに言及する、という点で、公衆衛生の定義に関連しており、社会的決定要因の有無は、‘人々が健康に過ごせる’環境に影響を及ぼす。[and whoseのandって必要無いような]
Social determinants can include such factors as the quality of housing, extent of community services, availability of transport, prospects for employment, crime levels, and access to parks, open space and suitable recreational facilities.
社会的決定要因は、住居の品質、地域サービスの広がり、移動手段の利用可能性、雇用の見通し、 危険水準、公園や広場、娯楽施設へのアクセスといったファクターからなる。
There are substantial and well-documented differences in health status between people who reside in upscale areas and those who reside in more deprived areas.
上流階層に属する人々とより低階層に属する人々の間の健康状況の違いは、膨大かつ詳細に記されている。
These contrasts have been documented in a number of countries and in a variety of cultures, although they have been best studied in the high-income countries (Kaplan, 1996).
これらの対比は、多くの国々、さまざまな文化で記されているが、最もよく研究されているのは、高所得国家である (Kaplan, 1996)。
The data show with remarkable consistency that people who live in the more affluent areas are invariably in better health than those from poorer areas, and this observation has endured well over time (Syme & Berkman, 1976; Kaplan et al., 1987; Marmot et al., 1987; Haan et al., 1989).
この資料は、注目すべき一貫性をもって、より裕福な地域に住む人々は、つねに、貧困地域に住む人々より健康であるということを、示しており、また、この観察は長年にわたり認められてきている (Syme & Berkman, 1976; Kaplan et al., 1987; Marmot et al., 1987; Haan et al., 1989)。
This finding is not dependent on how health status is measured, for it has been documented in terms of overall mortality, heart disease, diabetes or even subjective perceptions of ill-health (Pappas,1994; Blane, 1995; Kaplan et al., 1996; Link & Phelan, 1996; Goodman, 1999).
この発見は、全死亡率、心臓疾病、糖尿病あるいは健康障害の主観的知覚の点から記録されているため、どのように健康状況を評価したのか、には依存しない (Pappas,1994; Blane, 1995; Kaplan et al., 1996; Link & Phelan, 1996; Goodman, 1999)。
While there are numerous individual behavioral determinants involved in this profile (e.g. smoking, use of alcohol, quality of diet, regular exercise), there is also evidence that social determinants, i.e. those risk factors that apply to the whole community rather than to specific individuals, play a key role in determining health outcomes.
社会的決定要因は(喫煙、飲酒、食品の質、日常の運動といった)膨大な数の個人行動に関係しており、またヘルスアウトカムの決定に、重要な役割を演じている、という検証もある。そしてこれらは、特定の個人のみならず、地域全体に適応される。
When any of these basic community necessities are deficient or absent, the quality of life is diminished.
これらの地域の基本的要素のいずれかが、欠けたり不足したりすると、生活の質は低下する。
When they are mostly deficient, as is not uncommon in rundown parts of major cities, quality of life is diminished to the degree that a high level of emotional stress ensues from the demands of day-to-day coping with the cumulative burden of living in deprived circumstances.
これらがほとんど失われていた場合、これは大都市の荒れ果てた地区では珍しいことではないが、生活の質は低下し、貧困環境での生活による累積した重荷に対応する日々からくる高度な感情的ストレスが続く。
Poor social circumstances are linked to disease by way of material, psychosocial and behavioral pathways.
貧困な社会的環境は、物質的、心理社会的、行動的な経路により疾病と関係している。[P137で、それらの経路だけでは、説明できない、という記述がありましたが]
Social and environmental disadvantages can lead directly to poor health behavior and the subsequent biological disturbances that lead directly to ill-health.
社会的環境的不利は、不良な保健行動をもたらし、それに続く生物学的障害は、健康障害をもたらす。
This argument therefore holds that social stresses in themselves can negatively affect health (Brunner & Marmot, 1999).
従って、この議論は、社会的ストレスは健康に負の影響があるということを示す (Brunner & Marmot, 1999)。
As one example, the gap in both mortality rates and cardiovascular disease levels between Western European countries and those that were formerly part of the Soviet bloc were accentuated sharply around the time of the break-up of the Soviet Union.
1例として、西欧の国家と以前のSoviet圏の国家における、死亡率と心臓血管疾病の水準の格差は、Soviet連邦の崩壊前後から、急に目立った。
This phenomenon has been attributed to the high degree of social stress that accompanied the political break-up (Bobak & Marmot, 1996).
この現象は、政治的崩壊にともなう高度な社会的ストレスに原因がある (Bobak & Marmot, 1996)。
Dental research in this area has not developed to the extent it has in medical research, but there is some indication that the same relations between social determinants and oral health are generally evident.
この分野の歯科研究は、医科研究の広がりに発展していないが、社会的決定要因と口内保健の同じ関係が、一般に検証されているという示唆はある。
Parents’ employment status and attitudes have been identified as determinants of the dental health of young children in Belfast (Freeman et aI., 1997) and work stress was related to oral health among workers in Brazil (Marcenes & Sheiham, 1992).
Belfactでは、両親の雇用状況と態度は、若年者の歯科保健の決定要因であると、確認されており (Freeman et aI., 1997)、Brazilでは仕事のストレスは、職員の口内保健に関係していた (Marcenes & Sheiham, 1992)。
British studies, using a variety of measures to characterize the nature and extent of social deprivation in contrasting neighborhoods, have shown how the severity of dental caries is related both to the presence/absence of fluoridated drinking water (Chapter 18) and to the social deprivation level of the residential areas (Jones et al., 1997b, c; Jones & Worthington, 1999; Riley et al., 1999).
Britishの研究は、対照的な近隣地域の社会的剥奪の性質と広がりを示すさまざまな指標を利用して、フッ化物添加水道水の有無(18章)と居住地域の社会的剥奪水準が、齲蝕の重症度にどれだけ関係しているのか (Jones et al., 1997b, c; Jones & Worthington, 1999; Riley et al., 1999) を示している。
The effects of social inequalities in youth can be enduring; both low birthweight and social deprivation in youth are related to caries levels at age 13 years (Nicolau et al., 2003, 2005).
青年期の社会格差の影響は、永続的である。例えば、出生時体重の低さと青年期の社会的剥奪は、13歳の齲蝕水準と関係している (Nicolau et al., 2003, 2005)。[これは、life course analysisかな?]
Contrasts between social inequalities in youth are similarly related to caries severity in adolescence (Pattussi et al., 2001).
同じように、青年期の社会格差のコントラストは、青年期の齲蝕の重症度に関連している。
P139
These studies collectively demonstrate that dental caries today should be looked upon as a disease of poverty or deprivation as much as being a disease of diet, oral hygiene and other aspects of individual behavior.
これらの研究は、齲蝕は、食事、口内衛生、個人の行動のその他の側面による疾病である、というのと同じように、貧困や剥奪による疾病である、と見るべきである、ということを示している。
The great reductions in caries experience among more affluent people in the high-income countries stand in contrast to the much lower reductions in the more socially deprived groups.
高所得国家の裕福な人たちに生じている齲蝕経験の減少の大きさは、社会的剥奪集団における減少の小ささと対照的である。
Further advances in closing these disparities will require sweeping changes in social circumstances as much as changes in individual behavior.
これらの格差を解消するためには、個人の行動を変えるのと同じように、社会環境を大きく変えることが、必要である。
Since diet is a prime example of a personal behavior affected by neighborhood characteristics, its relationship to caries deserves some special attention.
食事は近隣特性により影響される個人行動の最たる例であるため、食事と齲蝕の関係には、特別な注意が向けられる。
Diet and dental caries
食事と齲蝕
Dietary practices are a complex mix of food availability, community and personal affluence, history, culture, marketing practices, and personal affluence, behavior and tastes.
食事は、利用可能な食品、地域の豊かさ、歴史、文化、販売活動、そして個人の豊かさ、行動、 嗜好の複雑な混合物である。[1つ目のand personalは誤植か]
Dietary quality is a major determinant of caries levels in a community, and is a major factor in the social environment.
食事の品質は、地域の齲蝕水準の主要な決定要因であり、社会環境における大きなファクターである。
The word diet refers to the food and drink that passes through the mouth, whereas nutrition is concerned with the absorption and metabolism of nutrients from dietary sources.
食事という言葉は、口を通過する食品と飲料水を意味するに対して、栄養は、食事から吸収され代謝される栄養物を意味する。
Although a link between malnutrition and caries would be intuitively expected, there is actually little evidence to support it.
栄養不良と齲蝕の関係は、直感的に予見されるが、実際にそれを支持する検証は、ほとんどない。
Studies of children in Peru have concluded that chronic and severe malnutrition during the first year of life is associated with increased caries years later, although this association is difficult to demonstrate because malnutrition delays eruption and exfoliation of the primary teeth (Alvarez, 1995).
栄養不良は乳歯の萌出と脱落を遅らせるので、この関係を示すのは難しいのだが、Peruの小児の研究は、出生後1年における、慢性かつ重度の栄養不良は、後年の齲蝕の増加と関係していると結論した (Alvarez, 1995)。
Chronic malnutrition among children in India has been shown to reduce salivary flow, which could be one reason for a causative link (Johansson et al., 1992).
Indiaの小児における慢性的な栄養不良は、唾液分泌を減少させることが示されているが、これが因果関係の理由の1つであろう (Johansson et al., 1992)。
By contrast, diet has a clear influence on caries development.
対照的に、食事は齲蝕進行に明らかな影響がある。
The relation between the intake of refined carbohydrates, especially sugars, and the prevalence and severity of caries is so strong that sugars are clearly a major etiological factor in the causation of caries.
精製された炭水化物、とりわけ砂糖と、齲蝕の広がりと重症度の関係は、強力であり、砂糖は明らかに齲蝕の因果関係における主要な病因ファクターである。
Added sugars are the primary culprit, although a limited degree of caries occurs in populations for whom the only sugars they consume are naturally occurring (Schamshula et al., 1978).
自然な量の砂糖を摂取する分には、それほどの齲蝕は生じず、添加した砂糖が、第一の原因である (Schamshula et al., 1978)。
While the evidence is strong that consumption of sugars is a major risk factor for caries, sugars are not the only food sources involved in the carious process.
砂糖の摂取は齲蝕の主要なリスクファクターであるという強力な検証がある一方で、砂糖は、齲蝕進行に関与する唯一の食品という訳ではない。
Cooked or milled starches can be broken down to low molecular weight carbohydrates by the salivary enzyme amylase and thus act as a substrate for cariogenic bacteria.
調理された、あるいは製粉されたでんぷんは、唾液酵素アミラーゼにより低い分子量の炭水化物まで破壊され、齲蝕原性微生物の基質となる。
It has long been asserted that sugar-starch mixtures are more cariogenic than sugars alone (Bibby, 1975), and there is some animal evidence to support that view (Firestone et al., 1984).
砂糖とでんぷんの混合物は、砂糖単体より齲蝕原性が強い (Bibby, 1975) と言われており、また、その視点を支持する動物実験もある (Firestone et al., 1984)。
The issue may never be totally clarified in humans, but it is reasonable and prudent to view all sugar-containing food and drinks, as well as cooked or milled starches, as potentially cariogenic.
このことは、ヒトで完全に解明されているのではないが、調理された、あるいは製粉されたでんぷんと、すべての砂糖含有食品や飲料水を潜在的に齲蝕原性であると考えることは、理にかなっているし、分別のあることである。
By contrast, the large molecular weight carbohydrates in lightly cooked vegetables are considered non-cariogenic because so little breakdown of these foods occurs in the mouth (Lingstrom et al., 2000).
それどころか、調理された野菜に含まれる分子量の大きい炭水化物は、口内で小さくなるまで咀嚼されるため、非齲蝕原性であると考えられている。
The evolving understanding of diet and caries
食事と齲蝕の進んだ理解
The great exploratory voyages of the seventeenth and eighteenth centuries led to the discovery of peoples previously unknown to Europeans, such as the islanders of the South Pacific, who appeared to live an idyllic life free of the diseases that afflicted Europe at the time.
17-18世紀の大航海時代は、当時の欧州を悩ませていた疾病もなく、牧歌的生活を営んでいるように見えるSouth Pacificの島民といった、以前のEuropansには知られていなかった人々の発見をもたらた。[未だに西洋圏は、meetではなくてdiscoveryと表現するんだな]
The concept of the ‘noble savage’ (Dubos, 1959) thus developed during the latter part of the eighteenth century.
この‘高潔なる野人’(Dubos, 1959) の概念は、18世紀後期に成立した。[Dubosも、言いたい放題だな]
An offshoot from this ideal was the belief that the apparent freedom from caries enjoyed by so-called ‘primitive’ races could be attributed to the ‘natural’ diet on which they existed.
この理想から、いわゆる‘原始’人が齲蝕からの自由でいられるのは、彼らの‘自然’食に理由がある、という考えが生じた。
Eating hard, fibrous and unprocessed food, so the theory went, led to better development of the jaws and teeth and helped to clear food debris from the teeth.
理論的には、硬く、繊維性で、加工されていない食品の摂取は、顎と歯の成長を促し、歯から食物残渣を取り除く助けとなる。
By contrast, Europeans were even then eating a lot of processed food, high in fermentable carbohydrates, which was thought to exercise the masticatory apparatus insufficiently and lead eventually to tooth decay.
対照的に、当時の欧州人は、大量の加工食品、過剰な発酵性炭水化物を摂取しており、咀嚼組織の運動は不十分であり、最終的に齲蝕となっていた。
Against the background of these beliefs, Miller, in the late nineteenth century, put forward his chemoparasitic theory of the development of dental caries.
このような考えを背景に、19世紀終わり頃、Millerは、齲蝕の進行についての化学的寄生物的理論を提示した。
Miller’s theory, developed during the ‘golden age of bacteriology’, was based on the action of microorganisms upon fermentable carbohydrates that adhered to the tooth’s surface (Miller, 1883).
Millerの理論は、‘微生物学の黄金期’に打ち立てられたが、歯面に付着した発酵性炭水化物上の微生物の活動に基づいていた。
Modern research shows that Miller got the overall picture pretty right.
現代の研究者は、Millerは全容をつかんでいたことを示している。
Theories about the preventive value of hard and fibrous foods became more widespread in the early twentieth century and became established dogma in many places.
硬い繊維性の食品による予防の価値についての理論は、20世紀早期に広まり、多くの地域でドグマが確立した。
One such article of faith stated that accumulations of fermentable carbohydrates could be removed by eating hard and fibrous foods (Wallace, 1902), the so-called ‘cleansing’ or ‘detersive’ foods.
このような信仰の1つとして、発酵性炭水化物の累積は、‘洗浄’あるいは‘洗剤’食品と呼ばれる、硬く繊維性の食品を摂取することにより除去される、という記載が残っている (Wallace, 1902)。
Another view was that if a meal was finished with a salivary stimulant such as an apple, the mouth would be kept free of fermentation both by the physical cleansing effect of the fibrous food and also because of the salivary flow induced by it (Pickerill, 1923).
もし、食事をりんごといった唾液刺激物で終えるなら、繊維性食品の物理的清掃効果と唾液分泌のため、口内では発酵が生じないだろう、といった視点もある。
However, ‘protective’ factors in a diet based on unprocessed foods have proven hard to identify.
しかし、非加工食品の‘保護’ファクターは、証明するのが難しい。
High-fiber diets with a good proportion of vegetables and fruit are today recommended by all health authorities, and these dietary guidelines are seen as promoting good oral health as well as general health.
野菜と果物の大部分は繊維性食品であり、今日、多くの保健当局により推奨されている。また、これらの食事指針は全身の健康と口内の健康を促進する。
Their value, however, is attributable less to the presence of hard and fibrous foods than to the relative absence of fermentable carbohydrates.
しかし、これら推奨は、硬く繊維性の食品であるということによるというよりは、発酵性炭水化物が入っていないということによるものである。
P140
In this historical context, the best known attempt to conduct an experimental study on the effect of diet on dental decay in humans was the Vipeholm study, conducted in Sweden between 1945 and 1952 (Gustafsson et al., 1954).
この歴史的背景で、ヒトの齲蝕への食事の影響についての実験研究を実施した、最も有名な企てが、Swedenで1945-1952年に実施されたVipeholm研究である (Gustafsson et al., 1954)。
The study was conducted in a mental institution (and by today’s standards it would be considered unethical because the participants were unable to give their informed consent to potentially harmful exposures).
この研究は、精神病院で実施された(今日の基準では、精神病院での研究は、被験者が害への曝露の可能性についてのインフォームドコンセントを与え[られ]ないので、非倫理的であると考えられる)。[because節のgiveって受動態じゃなくていいのか?]
Vipeholm’s conclusions profoundly influenced the way in which the role of sugars in dental decay was viewed, despite its complicated and flawed study design.
Vipeholmの結論は、その分かりにくさと、いまいちな研究デザインにもかかわらず、齲蝕における砂糖の役割の見方に大いに影響した。
In brief, inmates of the institution were divided into groups with controlled consumption of refined sugars which varied in amount, frequency, physical form, and whether they were taken with or between meals.
つまり、施設の入院患者は、いくつかの集団に分けられ、量、頻度、物理的形態、そして食事とともに摂るか、間食として摂るか、さまざまに精糖の摂取を管理された。
The extremes of intake were (a) no added sugars at all, to (b) daily between-meal consumption of 24 sticky toffees, each of which was too large to be swallowed and so had to be sucked and chewed.
摂取は (a) 砂糖を全く加えない、から (b) 毎日間食に大きすぎて飲み込めず、吸啜と咀嚼が必要な24のスティッキータフィーを摂取する、までであった。
The differences in caries incidence between the groups were pronounced, although
some of the Vipeholm conclusions can be challenged in the light of more recent research.
集団間の齲蝕発生の違いは顕著であったが、近年の研究は、Vipeholmの結果のいくつかに挑戦している。
Sugars-caries relationships in today’s low-caries environment
今日の低齲蝕環境における砂糖齲蝕関係
Many of the views on diet and caries are carry-overs from the pre-fluoride era, when caries was widespread and severe in high-income countries.
食事と齲蝕の視点の多くは、齲蝕が、高所得国家において蔓延し、重症化していた、フッ化物応用以前[前フッ化物時代]から、持ち越しされてきている。
In light of modern research protocols, design and analysis can be criticized in virtually all of them: all studies except for Vipeholm were cross-sectional, measurement of dietary intakes was often sloppy, and data analysis usually did not take likely confounders into account.
現代研究プロトコルの確立により、実質的にそのすべてのデザインと分析が、批判にさらされている。Vipeholm研究を除き、すべての研究が横断研究であり、食事摂取の評価がずさんであり、資料分析は交絡変数を計算に入れていなかった。
In the period of caries decline, however, researchers have to think that the ‘Vipeholm rules’ have changed.
しかし、齲蝕減少の時代では、研究者たちは、‘Vipeholmの法則’も真理ではなかった、と考えなくてはならない。
Are all the children with no detectable caries seen today not consuming sugar, or are other factors having a major influence?
今日をして、検出可能な齲蝕の無い小児は、砂糖を消費していないと、あるいは、その他のファクターが大きな影響を持っている、と言えるだろうか?
Studies such as those concluding that oral hygiene is an important covariable in the sugar-caries relationship (Hausen et al., 1981; Kleemola-Kujala & Rasanen, 1982;Sundin et al., 1992) have served to question the validity of the Vipeholm findings.
口内衛生は砂糖齲蝕関係の重要な共変量である (Hausen et al., 1981; Kleemola-Kujala & Rasanen, 1982; Sundin et al., 1992) と結論する研究者は、Vipeholmの法則の妥当性に一石を投じている。
Two prospective studies reported in the 1980s, one in Britain and one in the USA, measured diet and caries incidence concurrently and included more analytical detail than did any previous research.
1980年代に報告された2つの前向き研究は、1つはBritainで1つはUSAからであるが、食事と齲蝕の発生を同時に評価し、以前のどの研究よりも詳細に分析していた。
The British study followed 405 children with an average initial age of 11.5 years for 2 years (Rugg-Gunn et al., 1984).
Britishの研究は、開始時の平均年齢11.5歳の405人の小児を2年間追跡した (Rugg-Gunn et al., 1984)。
The children, all from a low-fluoride area near Newcastle, completed five food diaries, each for a 3-day period, for a total of 15 days of recorded diet over the 2 years.
Newcastle近くの低フッ化物地域の小児は、2年の間に、3日間の食事日記を5つ、合計15日分綴った。
Interviews with a dietitian followed each 3-day period to clarify uncertainties and to quantify amounts.
不確かな部分を確認し、量を定量化するために、3日間の後には、栄養士による面接を行った。
The mean DMFS incidence of the group was 3.63 over the 2 years, with 57% of new lesions in pits and fissures, a lower caries increment than the authors had expected.
2年間の集団のDMFS発生の平均値は3.63であり、新たなる病巣の57%の小窩裂溝であった。著者の予測より齲蝕の発生は少なかった。
Average consumption of all sugars was 118 g per day, providing 21% of energy intake.
砂糖消費の平均は、1日118gであり、エネルギー摂取の21%であった。
The results showed that caries increment was weakly but significantly correlated with total intake of sugars, but poorly correlated with frequency of intake.
結果は、齲蝕の増加と砂糖の摂取量の関連は弱いが有意であり、また摂取頻度との関連は不明であった。
The authors stated that because of the lower-than-expected caries increment, more clear-cut results would have been likely if the study had been extended for another year.
著者は、齲蝕の増加が予想より小さいため、より明瞭な結果のために、追跡の延長が必要であると結論した。
The second study was based in the low-fluoride area of Coldwater, Michigan, USA.
もう1つの研究は、USAのMichigan州Coldwaterの低フッ化物地域で行われた。
It followed 499 children, initially aged 11-15 years, for 3 years (Burt et al., 1988).
11-15歳の小児499人を3年間、追跡した (Burt et al., 1988)。
The majority completed four 24 h dietary recall interviews with a dietitian, although 27% completed more interviews.
大部分が、4回の栄養士による呼び出し面接を受けて24時間の食事日記を綴ったが、27%はより多くの面接を受けた。
The boys in the study averaged 156 g of sugar intake per day from all sources, the girls 127 g, and sugars accounted for 26% of total energy intake.
この研究で少年は1日平均156g、少女は127gの砂糖を、さまざまな形で摂取しており、また砂糖は総エネルギー摂取の26%を担っていた。
Both of these measures are higher than was found in the British group.
これらの水準は、Britishよりも高い。
Caries incidence, however, was lower than in the British group, averaging 2.9 DMF surfaces over the 3 years, of which 81% were pit-and fissure lesions (buccal pits and lingual extensions as well as occlusal lesions).
しかし、齲蝕の発生は、Britishよりも低く、3年で平均2.9DMF歯面であり、またその81%は裂溝病巣(咬合面と頬側小窩、舌側溝)であった。
Nearly 30% of the group developed no caries at all over the 3 years, and only 51 children (10.2%) developed two or more proximal lesions during the study.
約30%は、3年間で1本の齲蝕も発生せず、51人(10.2%)は2本以上の隣接面病巣を発生した。
Only among the latter ‘high-risk’ group was caries experience related to total intake of sugars, and that relationship was weak.
後者の‘ハイリスク’集団にのみ、齲蝕経験と砂糖の総摂取量の関係が見いだされたが、それもひ弱ものであった。
No relationships between caries experience and frequency of consumption were found.
齲蝕経験と摂取頻度に、何らかの関係は認められなかった。
The relative risk of caries from high sugar consumption relative to low sugar consumption was low (Burt & Szpunar, 1994); each additional 5g of sugars ingested daily was associated with a 1% increase in the probability of developing caries (Szpunaret al., 1995).
低摂取と比較した砂糖の過剰摂取による齲蝕の相対リスクは、低かった (Burt & Szpunar, 1994)。1日砂糖5gを追加摂取するは、齲蝕進行の可能性1%の上昇と関係があった (Szpunaret al., 1995)。
Despite some differences in study protocols, findings across these two independent studies were generally similar.
研究プロトコルに若干の違いはあるものの、これら2つの独立した研究から見いだされたことには、共通点がある。
Between them, the studies indicated that consumption of sugars is not a major risk factor for many children (i.e. those with no incident caries despite eating a lot of sugar), but it is for those who are still clearly susceptible to caries (broadly defined here as the minority who developed two or more proximal-surface lesions during the study).
両方の研究が、砂糖の消費は、多くの小児にとっては、大きなリスクファクターではない(つまり、砂糖の取り過ぎにもかかわらず、齲蝕発生が無い)が、齲蝕感受性のある(2本以上の隣接面病巣を進行した一部の)小児にとっては、大きなリスクファクターであることを示唆していた。
A systematic review of the present-day caries-sugars relationship (Burt & Pai, 2001) also concluded that the sugar-caries relationship was not as strong as generally supposed.
今日の齲蝕砂糖関係についてのシステマティックレビュー (Burt & Pai, 2001) も、砂糖齲蝕関係は一般に考えられているほど強力ではない、と結論している。
This report identified 36 studies since 1980, all conducted in countries where there is wide scale exposure to fluoride, which met the quality criteria for inclusion in the review.
このシステマティックレビューは1980年以後の、フッ化物への大規模な曝露のある国々で行われた、レビューの品質基準を満たした、36の研究を調べていた。
Eighteen of these studies found only a weak relationship between sugar consumption and incident caries, 16 found a moderate relationship and only two identified a strong relationship.
これらの研究の18は、砂糖の消費と齲蝕の発生に弱い関連を見いだしており、16が中程度の関係、2本が強力な関係を見いだしていた。
The evidence from these more recent studies suggests that sugars still play a modest role as a risk factor for caries, especially among more high-risk children, but that this relationship is by no means linear.
これら、より近年の研究は、砂糖は齲蝕のリスクファクターとしては、とりわけハイリスク小児において、穏やかな役割を演じているが、 決して線形の関係があるわけではないことを、示唆している。
P141
The much stressed role of frequency of consumption of sugars (‘it’s not how much you eat, it’s how often you eat it’) is clearly questioned by the results of the Newcastle and Michigan studies, as it has been by other studies in Sweden (Sundin et al., 1983; Bergendal & Hamp, 1985; StecksenBlickset al., 1985).
NewcastleとMichiganの研究の結果から、またSwedenの別の研究結果から、砂糖の摂取頻度の役割(‘摂取量ではなく、摂取頻度’)が強調された (Sundin et al., 1983; Bergendal & Hamp, 1985; StecksenBlickset al., 1985)。
The importance of frequency of consumption was a major finding of the Vipeholm study, and it has been prominent in dental health education ever since.
摂取頻度の重要性は、Vipeholm研究の成果であり、その後の歯科保健教育に卓越した影響をもたらした。
However, the importance of frequency in Vipeholm was principally based on the caries experience of the group which consumed 24 large toffees between meals each day, a frequency of consumption that was not even approached in either the British or the Michigan study.
しかし、Vipeholmで重要視された摂取頻度は、第一に、BritishやMichigan研究のどちらでもアプローチしなかった摂取頻度である、毎日の間食に、24の大トフィーを摂取した集団の齲蝕経験に基づいていた。
The results from the highly artificial circumstances and non-representative sample of the Vipeholm study thus may be misleading when generalized to the population at large.
Vipeholm研究の、高度に人工的な環境の結果と非代表標本は、大規模な集団に適応すると、誤解をまねく。
Even so, frequency and amount of fermentable carbohydrate are related, and this issue has come to light again with recent evidence on the role of soft drinks in caries development.
とはいえ、発酵性炭水化物の摂取頻度と摂取量は関連しており、また、この論点は、齲蝕進行における清涼飲料水の役割についての近年の検証により、再び脚光を浴びるようになっている。
Caries and soft drinks
齲蝕と清涼飲料水
Sugar in liquid form is cariogenic; it served well to demonstrate demineralization in landmark experimental caries studies (Van der Fehr et al., 1970).
飲料水中の砂糖は、齲蝕原性である。飲料水中の砂糖のすぐれた脱灰作用は、歴史に残った、かの実験的齲蝕研究にて示されている (Van der Fehr et al., 1970)。
There is more recent evidence to show that soft drink consumption is related to caries: the more often soft drinks are consumed, the greater the extent and severity of caries (Ismail et al., 1984; Jones et al., 1999; Watt et al., 2000; Marshall et al., 2003).
清涼飲料水の消費は齲蝕に関連している、というより近年の検証がある。清涼飲料水の消費頻度が上昇すると、齲蝕の広がりと重症度は悪化する (Ismail et al., 1984; Jones et al., 1999; Watt et al., 2000; Marshall et al., 2003)。[なにも4つも引用せんでも、いいだろうに...]
Soft drinks have also been implicated as part of the cause of the global epidemic of obesity in children (Mann, 2003), for it is now common to find soft drinks and juices replacing formula and milk in children up to 2 years of age (Marshall et al., 2003).
今や、清涼飲料水のたぐいは、乳幼児が2歳になると乳児用ミルクやミルクと置き換わる時代 (Marshall et al., 2003) なので、小児の肥満の世界的な地域的流行の原因の1つと目されている (Mann, 2003)。[endemic局地的、epidemic地域的、pandemic世界的ですが...global epidemicとは、これ如何に...]
A study among low-income adults found that 54% of their total energy intake came from several types of soft drinks and juices, and that high consumption of soft drinks when linked to poor oral hygiene was associated with higher caries levels (Burt et al., 2006).
低所得の成人の研究は、彼らは、総エネルギーの54%を清涼飲料水のたぐいから摂取しており、清涼飲料水の過剰摂取と不良な口内衛生は、高水準の齲蝕と関連がある (Burt et al., 2006)。
Soft drinks seem to have replaced confectionery as the prime source of sugar in several populations.
清涼飲料水は、いくつかの集団では、お菓子の代わりとして、砂糖の主たる摂取源に置き換わっているようだ。
The subject therefore has serious health implications that go beyond dentistry, and is yet another example of a general public health problem having clear dental overtones.
だから、この件は、歯科を越えた保健上の重大な示唆があり、かつ、歯科的色彩を持つ公衆衛生的疾病の1例である。
Soft drinks thus can be viewed as a ‘common risk factor’ in public health (Sheiham & Watt, 2000).
そういうわけで、清涼飲料水は、公衆衛生における‘共通のリスクファクター’とみなされる (Sheiham & Watt, 2000)。
P141
Summary
まとめ
The epidemiology of caries has traditionally been expressed in terms of bad diet, poor oral hygiene, cariogenic bacteria in plaque, ‘acid attacks’ and demineralization, salivary flow and exposure to fluoride.
従来より、齲蝕の疫学は、悪い食事、悪い口内衛生、プラーク中の齲蝕原性細菌、‘酸の攻撃’と脱灰、唾液の流量とフッ化物への暴露の観点から、語られてきている。
Those factors and others are all part of how and why caries develops, but this is too narrow a view for full understanding of the disease.
これらの要因は、すべて、齲蝕の進行の仕組みや理由の一部であるが、視野が狭すぎて、すべてを理解するには至らない。
In recent years there has been a growing awareness that there is a wider social dimension to caries, just as there is with other diseases.
近年、齲蝕には、ちょうど他の疾病と同じように、さまざまな社会的要因がある、ということに注意が向けられてきている。
The growth of social and lifecourse epidemiology has shown the importance of the social environment in caries, and how youthful influences can years later affect adult disease.
社会疫学により、齲蝕における社会環境の重要性が明らかとなり、ライフコース疫学により、若年期がどれほど成人期の疾病に影響をもたらすのかが、明らかとなっている。
A comprehensive view of caries epidemiology includes all environments, from those at the plaque-enamel interface to the social environment in which a person lives.
齲蝕の疫学の包括的視点は、プラーク-エナメル界面から、その人の生活している社会環境までの、あらゆる環境からなる。
Caries is a disease of social deprivation, just as it is a disease of bad diet (indeed, those two factors are frequently found together).
齲蝕は社会的剥奪をもたらす疾病であり、また食生活を悪化させる疾病である(実際、これら2つのファクターは、しばしば併発する)。
The key to eventual control of caries thus lies in improving the broad social environment for affected populations just as much as it does in intervening to improve the intra oral environment.
だから、齲蝕管理の究極の鍵は、口内環境の改善を目的とした介入と、集団に影響をもたらすさまざまな社会環境の改善にある。[疫学の章なのに、まとめは齲蝕管理になっている不思議...][2010.3.11]
References
Boxs 8.1-4
Box 8.1 Properties of an ideal index
Box 8.1 理想的な指数の性質
・Validity. The index must measure what it is intended to measure, so it should correspond with clinical stages of the disease under study at each point.
・妥当性 指数は、目的としているものを評価しなければならず、だから、疾病の臨床ステージに一致すべきである。
・Reliability. The index should be able to measure consistently at different times and under a variety of conditions.
・信頼性 指数は何度やっても、どのような条件の元でも、矛盾無く[疾病を]評価できるべきである。[あれ?measureが自動詞になってるような..]
The term reliability is virtually synonymous with reproducibility, repeatability and consistency, meaning the ability of the same or different examiners to interpret and use the index in the same way.
信頼性という用語は、再現性や一貫性と実質的には同意である。同じ、あるいは異なる検査者が、同じように指数を読み取り利用できる能力を意味している。
・Clarity, simplicity and objectivity. The criteria should be clear and unambiguous, with mutually exclusive categories.
・明瞭で平易、かつ客観的 基準は、相互排他的で明確で曖昧さのない区別であるべきである。
Ideally, it should be readily memorized by an examiner after some practice.
ある程度の訓練で検査できるようになる指数であれば、理想的である。
・Quantifiability. The index must be amenable to statistical analysis, so that the status of a group can be expressed by a distribution, mean, median or other statistical measures.
・計量可能性 集団の状況は、分布、平均値、中央値、その他の統計的評価により表現できるように、指数は統計的分析が可能でなければならない。
・Sensitivity. The index should be able to detect reasonably small shifts, in either direction, in the condition.
・感度 指数は、いずれの方向であれ、適度に小さな変化を検出可能であるべきである。
・Acceptability. The use of the index should not be painful or demean-ing to the subject.
・受容性 指数の使用により、被験者に痛みや屈辱を与えるべきではない。
Box 8.2 Limitations of the DMF index
Box 8.2 DMF指数の欠点
The DMF index has received remarkably little challenge over some 70 years of life, probably because it is conceptually simple and versatile in practice.
DMF指数は70年にわたり、大きな変化はほとんどない。多分、その概念的なシンプルさと融通のよさによるものだろう。
But it was developed for use in children a long time ago, and accordingly it shows its age in a few areas.
だが、DMF指数は、むかしむかしの小児に適応するために開発されたものであり、それゆえ、いくつかの地区では小児を表す。
The principal limitations of the DMF index are:
さて、その主たる欠点をあげつらおう。
・DMF values are not related to the number of teeth at risk.
・DMF値は、リスクにある歯の数とは関係がない。
A DMF score for an individual is a simple count of those teeth that in the examiner’s judgment have been affected by caries; it has no denominator.
個人のDMFスコアは、検査者により齲蝕経験があると判断された歯をカウントする。そして、分母がない。
A DMF score thus does not directly give an indication of the intensity of the attack in anyone individual.
DMFスコアは、個人の攻撃の熾烈さの目安には、直接には、ならない。
A 7-year-old child with a DMF score of 3.0 may have only nine permanent teeth in the mouth; thus, one-third of these teeth have already been attacked by caries in a short space of time.
DMFスコア3.0の7歳児は、口内に9本の永久歯しかない、かもだ。だから、たったの7歳で、歯の1/3が齲蝕に侵されたことになる。
An adult may have a DMF score of 8.0 from a full complement of 32 teeth; thus, over a longer period only one-quarter of the teeth have been affected.
DMFスコア8.0の成人は、口内に32本の歯を持つ、かもだ。だから、長い人生で歯の1/4のが齲蝕に侵されたことになる。
DMF scores therefore have little meaning unless age is also stated.
お分かりかな。DMFスコアは、年齢が分からなければ、意味がないのだ。[それって、偉そうにあげつらうほどの欠点か?]
・The DMF index gives equal weight to missing , untreated decayed or well-restored teeth.
・DMF指数は、喪失歯、未治療歯、修復歯を同等に評価する。
Common sense suggests that this philosophical basis is faulty for many purposes.
常識によれば、この哲学は多くの目的にあっていない。
・The DMF index is invalid when teeth have been lost for reasons other than caries.
・DMF指数は、齲蝕ではない理由で失った歯がある場合には、妥当性を失う。
Teeth can be lost for periodontal reasons in older adults, and for orthodontic reasons in teenagers.
歯は、高齢者なら歯周疾病で失うこともあれば、10代でも矯正治療で失うこともある。
Decision rules, which go along with criteria, are required to determine how to deal with these instances.
決定基準は、これらの場合をどのように扱うのかを決定しなければいけない。
・The DMF index can overestimate caries experience in teeth with ‘preventive restorations’.
・DMF指数は、‘予防修復’歯を齲蝕経験として、過大に評価する。
In an epidemiological survey, such teeth must be included in the F component of DMF, although had they not been filled in the first place they might have been diagnosed as sound teeth.
疫学調査では、予防修復歯は、DMF要素のFに加算されるが、もしも修復されていないなら、健全歯と診断されただろう。
DMF scores will thus be inflated (Bader et al., 1993).
DMFスコアは、このように、水増しが生じうる (Bader et al., 1993)。
Composite restorations judged to have been placed only for cosmetic reasons likewise should not be included in DMF counts.
同様に、審美的理由だけでなされたと思われるコンポジット修復は、DMFカウントに含まれるべきではない。
・Composite and resin restorations not only may have been placed on non-carious teeth, but are often hard for an examiner to detect, thus leading to underestimation.
・コンポジットレジンは、齲蝕のない歯を修復するだけではなく、検出しにくいため、過小評価の原因となる。
・DMF scores cannot be compared from one group to another without considering the criteria by which caries was considered present or absent.
・異なる集団のDMFスコアは、齲蝕の判断基準を考慮せずには、比較することはできない。
There is no universal criterion for what is a decayed tooth.
う歯の判断基準は、普遍的ではない。
Comparing one group where caries was recorded across the full disease continuum to one which only recorded caries at cavitation is clearly invalid.
あらゆる齲蝕を齲蝕として記録する集団と、齲窩のある齲蝕のみを齲蝕として記録する集団を比較することは、あきらかに妥当ではない。
・DMF data are of little use for estimating treatment needs.
・DMFの資料は、治療のニーズの推定には使えない。
・DMF cannot account for sealed teeth.
・DMFは、シーラントをカウントしない。
Sealants did not exist in 1938, so are obviously not included in the description of the index.
1938年以前にはシーラントは存在しなかったため、DMF指数には含まれていない。
Sealants and other composite restorations for cosmetic purposes have to be dealt with separately.
シーラントと審美コンポジット修復は、別々に扱わなくてはならない。
Box 8.3 Typical criteria for diagnosing caries through the full range of lesion development (the D1-D3 scale), shown to contrast with the criteria for diagnosis at the dentinal-Iesion stage only (the dichotomous scale)
Box 8.3 D1-D3尺度(病巣のあらゆる進行段階を齲蝕と診断)と2点尺度(象牙質病巣のみを齲蝕と診断)との比較。
Diagnosis through the full range of caries; the D1-D3 scale
あらゆる進行段階の診断; D1-D3尺度
O. Surface sound. No evidence of treated or untreated clinical caries (slight staining allowed in an otherwise sound fissure).
O. 健全歯面 治療痕や未治療の齲蝕がない(健全な裂溝のわずかな着色は許容する)。
D1. Initial caries. No clinically detectable loss of substance.
D1. 初期齲蝕 臨床的に検出可能な実質欠損がない。
For pits and fissures, there may be significant staining, discoloration or rough spots in the enamel that do not catch the explorer, but loss of substance cannot be positively diagnosed.
小窩裂溝のエナメル質に、探針では触知しない、着色、変色、あるいはざらついた点があるものの、実質欠損は認められない。
For smooth surfaces, these may be white, opaque areas with loss of luster.
平滑面では、これらは光沢を失い、透明感のない白さとなる。
D2. Enamel caries. Demonstrable loss of tooth substance in pits or fissures, or on smooth surfaces, but no softened floor or wall or undermined enamel.
D2. エナメル質齲蝕 小窩裂溝あるいは平滑面に実質欠損はあるが、軟化した窩底や壁、脆いエナメル質はない。
The texture of the material within the cavity may be chalky or crumbly, but there is no evidence that cavitation has penetrated the dentin.
齲窩に面した歯質のテクスチャーは、チョーク様あるいは砕けやすいが、象牙質まで侵されているという感じではない。
D3. Caries of dentin. Detectably softened floor, undermined enamel or a softened wall, or the tooth has a temporary filling .
D3. 象牙質齲蝕 軟化した窩底、脆いエナメル質、軟化した窩壁を検出可能、あるいは、仮充填のある歯。
On approximal surfaces, the explorer point must enter a lesion with certainty.
隣接面では、探針が病巣にしっかりと入る。
D4. Pulpal involvement. Deep cavity with probable pulpal involvement.
D4. 歯髄侵襲性 歯髄侵襲をともなう、深い齲窩。
Pulp should not be probed (Usually included with D3 in data analysis.)
歯髄は調べるべきではない(通常D3に含めてしまう)。
Diagnosis at the dentinal lesion stage only; the dichotomous scale
象牙質病巣の段階でのみ診断; 2点尺度
Pits and fissures on the occlusal, vestibular and lingual surfaces are carious when the explorer ‘catches’ after insertion with moderate to firm pressure and when the ‘catch’ is accompanied by one or more of the following signs of decay:
咬合面、頬側面、舌側面の小窩裂溝に、圧力を安定させるため探針を穏やかに挿入し、以下の兆候が1つ以上認められれば、齲蝕と診断する。
・softness at the base of the area
・その部分の底が軟化している。
・opacity adjacent to the areaa provides evidence of undermining or demineralization
・その部分に隣接した不透明部分aが蝕まれ、脱灰を呈している。
・softened enamel adjacent to the area that may be scraped away by the explorer.
・探針により破壊された部分に隣接した軟化エナメル質。
a These areas should be diagnosed as sound when there is apparent evidence of demineralization, but no evidence of softness.
a これらの領域が、再石灰化が明らかであり、かつ、軟化が認められなければ、健全であると診断される。
Source: Pitts & Fyffe (1988), Horowitz (1972) and WHO (1979).
Box 8.4 Reasons why the DMF index is of limited value in measuring the treatment needs of a population
Box 8.4 DMF指数が、集団の治療ニーズの評価としては使えない理由。
・ Criteria used to diagnose caries in a survey usually are not the same as those used by practitioners in forming a patient’s treatment plan.
・調査における齲蝕の診断基準は、通常、臨床家が患者の治療計画の立案において利用する齲蝕の診断基準とは違う。
For example, a practitioner has to judge whether a minor lesion will develop into a major lesion over time, and whether a lesion in a primary tooth can safely remain untreated for the life of the tooth.
たとえば、臨床家は、将来、小さな病巣は大きな病巣になるかどうか、また乳歯の病巣は、脱落するまで治療しなくても心配ないかどうか、を判断しなければいけない。
A survey scores a tooth by how it appears at the present time.
調査では、現在、どのような状態であるかを、スコアリングする。
・ Patients’ own perceived needs, level of interest in their dental conditions and ability or willingness to pay, all influence the level of treatment carried out.
・患者自身の認知したニーズや、歯の状況と能力についての興味の水準、あるいは支払いへの乗り気は、全て、行われる治療の水準に影響する。[percieved needsはneedsの概念の一部です]
These factors are not part of survey data,
これらのファクターは、調査資料には含まれない。
・ Treatment philosophies change with expanding knowledge and technological developments; a treatment that is standard today may not be so tomorrow.
・治療哲学は、知識の広がりと技術的進歩により変化する。今日の標準治療は、明日には、そうではないかもしれない。
References
Alvarez JO. Nutrition, tooth development, and dental caries. Am J ClinNutr 1995; 61: 410-16S.
Anderson RI. Bradnock G, lames PMC. The changes in the dental health of 12-year-old school children in Shropshire. Br Dent I 1981; 150:278-81.
Athanassouli I, Mamai-Homata E, Panagopoulos H, Koletsi-Kounari H. Apostolopoulos A. Dental caries changes between 1982 and 1991 in children aged 6-12 in Athens, Greece. Caries Res 1994; 28: 378-82.
Backer-Dirks 0, Houwink B. Kwant GW. The results of 6½ years of artificial drinking water in the Netherlands; the Tiel-Culemborg experiment.Arch Oral Bioi 1961; 5: 284-300.
Bader JD, Shugars DA. What do we know about how dentists make caries-related treatment decisions? Community Dent Oral Epidemiol1997; 25:97-103.
Bader JD, Shugars DA, Rozier RG. Relationship between epidemiologic coronal caries assessments and practitioners’ treatment recommendations in adults. Community Dent Oral Epidemiol1993; 21: 96-101.
Baelum V, Fejerskov 0, Manji F. The ‘natural history’ of dental caries and periodontal diseases in developing countries: some consequences for health care planning. Ti:mdlaegebladet 1991; 95: 139-48.
Barnard PD. Tamworth dental survey, summary report 1963-1988.Westmead, Australia: Westmead Centre for Ora) Health, 2005.
Beal ]E The dental health of five-year-old children of different ethnic originsresident in an inner Birmingham area and a nearby borough. ArchOral Bioi 1973; 18: 305-12.
Beck ID. The epidemiology of root surface caries: North American studies. Jldv Dent Res 1993; 7: 42-51.Beck ID. Risk revisi ed. Community Dent Oral Epidemiol1998; 26: 220-5.
Beltnln-Aguilar EO, Barker LK, Canto MT, et al. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis - United States, 1988-1994 and 1999-2002. MMWR 2005;54(SS-3): 1-44.Bergendal
B, Hamp SE. Dietary pattern and dental caries in 19-year-oldadolescents subjected to preventive measures focused on oral hygieneand/or fluorides. Swed Dent J 1985; 9: 1-7.
Bibby BG. The cariogenicity of snack foods and confections. JAm DentAssoc 1975; 90: 121-32.
Bjarnason S, Kohler B, Ranggard L. Dental caries in a group of 15 to16-year-olds from Goteborg. Part 1. Swed Dent J 1992; 16: l43-9.
Bjarnason S, Finnbogason SY. Holbrook P, Kohler B. Caries experience inIcelandic 12-year-old urban children between 1984 and 1991.Community Dent Oral Epidemiol1993; 21: 195-7.
Blane D. Social determinants of health - socioeconomic status, social class,and ethnicity. Am I Public Health J995; 85: 903-5.
Bobak M, Marmot MG. East-West mortality divide and its potential explanations:proposed research agenda. BM! 1996; 312: 421-5.
Bohannan HM. Caries distribution and the case for sealants. J Public Health Dent 1983; 43: 200-4.
Bratthall D. Introducing the Significant Caries Index together with a proposal for a new oral health goal for 12-year-olds, lilt Dent! 2000; 50: 378-84.
BratthaJl D, Hansel Petersson G, Sundberg H. Reasons for the cariesdecline: what do the experts believe? Eur! Oral Sci 1996; 104: 416-22.
Brown loJ, Kingman A, Brunelle lA, Selwitz RH. Most US schoolchildren are caries free in their permanent teeth: this is no myth. Public HealthRep 1995; 110: 531-3.
Brunner E, Marmot MG. Social organization, stress, and health. rn:Marmot M, Wilkinson RG, eds. Social determinants of health. New York:Oxford University Press, 1999: 17-43.
Bryan ET, Collier DR, Vancleave M1. Dental health status of children inTennessee; a 25-year comparison. JTerm Dent Assoc 1982; 62: 31-3.
Burt BA. Influences for change in the dental health status of populations: an historical perspective. J Public Health Dent 1978; 38: 272-88.
Burt BA. The future of the caries decline. J Public Health Dent 1985; 49:368-76.
Burt BA, Pai S. Sugar consumption and caries risk: a systematic review. J Dellt Educ 2001; 65: 1017-23.
Burt BA, Szpunar SM. The Michigan Study: the relationship between sugars intake and dental caries over three years. Int Dent] 1994; 44:230-40.
Burt BA, Ismail Al, Eklund SA. Root caries in an optimally-fluoridated and a high-fluoride community. JDent Res 1986; 65: 1154-8.
Burt BA, Eklund SA, Morgan Kl, et al. The effects of sugars intake and frequency of ingestion on dental caries increment in a three-year longitudinal study.] Dent Res 1988; 67: 1422-9.
Burr BA, Kolker llo, Sandretto AM, Yuan Y, Sohn W, Ismail AI. Dietary patterns related to caries in a low-income adult population. Caries Res2006; 40: 473-80.
Carmichael CL, Rugg-Gunn AJ, Ferrell RS. The relationship between fluoridation, social class and caries experience in 5-year-old children in Newcastle and Nortl1umberland in 1987. Br Dent] 1989; 167: 57-6l.
Carvalho IC, Van Nieuwenhuysen lP, D'Hoore W. The decline in dental caries among Belgian children between 1983 and 1998. CommunityDell1 Oral Epidemiol200 I; 29: 55-6l.
Caufield PW, Dasanayake AP, Li Y, Pan Y, Hsu I, Hardin jM. Natural historyof Streptococcus sanguinis in the oral cavity of infants: evidence for a discrete window of i.nfectivity. InJeet 1111111un 2000; 68: 4018-23.
Chalmers IM, Carter KD, Fuss JM, et al. Caries experience in exissting and new nursing home residents in Adelaide, Australia. Gerodontology 2002;19: 30-40.
Chen M, Andersen RM, Barmes DE, Leclerq M-H, Lyttle Se. Comparingoral health systems. A second international collaborative study. Geneva:World Health Organization, 1997.
Chironga L, Manji F. Dental caries in 12-year-old urban and rural children in Zimbabwe. Community Dent Oral Epidennol1989; 17: 31-3
Corbelt ME, Moore Wl. Distribution of dental caries in ancient Britishpopulations. [V: The 19th century. Caries Res 1976: 10: 401-14.
Dean HT, Arnold FA I r, Elvove E. Domestic water and dental caries. V.Additional studies of the relation of fluoride domestic waters to dental caries experience in 4.,425 white children aged 12-14 years of age in 13cities in 4 states. Public Health Rep 1942; 57: 1155-79.
DePaola PF, Soparkar PM, Tavares M, Kent RL lr. The clinical profiles of individuals with and without root caries. Gerodontology 1989; 8: 9-16.
Downer Me. Caries prevalence in the United Kingdom. 1nl Dent] 1994;44(Suppl 1): 365-70.
Drake CW, Hunt RI, Beck lD, Koch GG. Eighteen-month coronal caries incidence m North Carolina older adults. ] Public Health Dent 1994; 54:24-30.
Dubos R. The mirage of health. New York: Doubleday, 1959.Espelid I, Tveit AB, Haugejorden 0, H.iordan Pl. Variation in radiographic interpretation and restorative treatment decisions on approximal caries among dentists in Norway. Community Dent Oral EpidemJOI 1985; 13:26-9.
Fejerskov 0, Antoft P, Gadegaard E. Decrease in caries experience in Danish children and young adults in the 1970s. ] Dent Res 1982; 61 (Special Issue): 1305-10.
Firestone AR, Schmid R, Miihlemann HR. Effect on the length and number of intervals between meals on caries in rats. Caries Res 1984; 18:128-33.
Flinck A, Kallestal C. Holm AK, Allebeck P, Wall S. Distribution of cariesin 12-year-old children in Sweden. Social and oral health-related behaviouralpatterns. Community Dent Health 1999; 16: 160-5.
Freeman R, Breistein B, McQueen A, Stewart M. The dental llealth statusof five-year-old children in north and west Belfast. Community DentHealth 1997; 14: 253-7.
Freire M, Hardy R, Sheiham A. Mothers' sense of coherence and their adolescent children's oral health status and behaviours. Community DentHealth 2002; 19: 24-31.
Fuchs V. Who shall live? Health, economics, and social choice. New York:Basic Books, 1974.Gilbert GH, Duncan RP, Dolan TA, Foerster U. Twenty-four month incidence of root caries among a diverse group of adults. Caries Res 2001;35: 366-75.
Glass Rl.. Secular changes in caries prevalence in two Massachusetts towns.Caries Res 1981; 15: 445-50.
Goodman E. The role of socioeconomic status gradients in explainingdifferences in US adolescents' health. Am ! Public Health 1999; 89:1522-8.
Grainger RM. Epidemiological data. [n: Chilton NW, ed. Design andanalysis in dental and oral research, 1st edn. Philadelphia, PA:Lippincott, 1967: 311-53.
Gratrix 0, HoJloway Pl. Factors of deprivation associated with dental caries in young children. Community Dent Health 1994; 11: 66--70.
Graves RC, Bohannan HM, Disney lA, Stamm lW, Bader lD,Abernathy lR.Recent dental caries and treatment patterns in US children. J PublicHealth Dent 1986; 46: 23-9.
Gray M, Morris AI, Davies, l. The oral health of South Asian five-year-old children in deprived areas of Dudley compared with white children of equal deprivation and fluoridation status. Community Dent Health2000; 17: 243-5.
Gustafsson BE, Quensel C-E, Swenander Lanke L, et al. The Vipeholm dental caries study. The effect of different levels of carbohydrate intake on caries activity in 436 individuals observed for five years. Acta OdontScand 1954; 11: 232-364.
Haan MN, Kaplan GA, Syme S1. Socioeconomic status and health: oldobservations and new thoughts. In: Bunker lP, Gomby DS, Kehrer BH,eds. Pathways to health: the role oJsocial factors. Menlo Park, CA: Henry 1Kaiser Family Foundation, 1989: 76-135.
Hadden We. The use of educational attainment as an indicator of socioeconomic position. Am! Public Health 1996; 86: 1525-6.
Hand JS, Hunt RJ, Beck lD. Incidence of coronal and root caries in an older adult population. J Public Health Dent 1988; 48: 14- J9.
Hargreaves lA, Wagg BI, Thompson GW. Changes in caries prevalence ofIsle of Lewis children, a historical comparison from 1937 to 1984. CariesRes 1987; 21: 277-84.
Hausen H, Heinonen OP, Paunio 1. Modification of occurrence of caries in children by toothbrushing and sugar exposure in fluoridated and nonfluoridated areas. Community Dent Oral Epidemiol 1981; 9: 103-7.
Hawkins RI, Main PA, Locker D. Oral health status and treatment needs of Canadian adults aged 85 years and over. Special Care Dent 1998; 18:164-9.Horowitz HS. Clinical trials of preventives for dental caries. ] Public HealthDent 1972; 32: 229-33.
Hughes JT, Rozier RG. The survey of dental health in the North Carolinapopulation; selected findings. In: Bawden JW, De Friese GH, eds. Planning Jor dental care on a statewide basis; the North Carolina dental manpower project. Chapel Hill, NC: Delltal Foundation of NorthCarolina, 1981: 21-37.
Hugoson A, Koch G, Hallonsten A-lo, Ludvi.gsson N, Lundgren D,Rylander H. Dental health 1973 and 1978 in individuals aged 3-20 years in the community of Jonkopping, Sweden. Swed Dent] 1980; ISO: 217-29.
Hunter PBV. The prevalence of dental caries in 5-year-old New Zealandchildren. NZ Dent] 1979; 75: 154-7.
Institute of Medicine. The future of public health. Washington DC: National Academy Press, 1988.Ismail AI, Burt BA, EkJund SA. The cariogenicity of soft drinks in theUnited States. JAm Dent Assoc 1984; 109: 241-45.
Ismail AI, Brodeur JM, Gagnon P, et al. Prevalence of non-cavitated and cavitated carious lesions in a random sample of 7-9-year-old schoolchildrenin Montreal, Quebec. Community Dent Oral Epidemiol 1992;20: 25
Johansson I, Saellstrom AK, Rajan BP, Parameswaran A. Salivary flow and dental caries in Indian children suffering from chronic malnutrition.Caries Res 1992; 26: 38-43.
Jones CM, Worthington H. The relationship between water fluoridation and socioeconomic deprivation on tooth decay in 5-year-old children. Br Dent! 1999; 186: 397-400.
Jones C, Taylor G, Woods K, Whittle G, Evans D, Young P. Jarman underprivileged area scores, tooth decay and the effect of water fluoridation. Community Dent Health 1997a; 14: 156-60.
Jones CM, Taylor GO, Whittle IG, Evans D, Trotter Or. Water fluoridation, tooth decay in 5 year olds, and social deprivation measured by thelarman score: analysis of data from British dental surveys. BM! 1997b;315: 514-17.
Jones CM, Woods K, Taylor GO. Social deprivation and tooth decay in Scottish schoolchildren. Health Bull 1997c; 55: 11-15.
Jones C, Woods K, Whittle G, Worthington H, Taylor G. Sugar, drinks, deprivation and dental caries in 14-year-old children in the north west of England in 1995. Community Dent Health 1999; 16: 68-71.
Kallestal C, Wall S. Socioeconomic effect on caries. Incidence data among Swedish 12-14-year-ol.ds. Community Dent Oral Epldemiol 2002; 30:108-14.
Kaplan GA. People and places: contrasting perspectives on the association between social class and health.lnt f Health Serv 1996; 26: 507-19.
Kaplan GA, Haan MN, Syme SL, Minkler M, Winkelby M. Socioeconomic status and health. In: Amler RW, Dull HB, eds. Closing the gap: the burdenof unnecessary illness. New York: Oxford University Press, 1987: 125-9.
Kaplan GA, Pamuk E, Lynch JW, Cohen RD, Balfour IL. Inequality in income and mortality in the United States: analysis of mortality and potential pathways. BM! 1996; 312: 999-1003.
Kaste LM, Selwitz RH, Oldakowski RJ, Brunelle lA, Winn DM, Brown LI. Coronal caries in the primary and permanent dentition of children and adolescents 1-17 years of age: United States, 1988-1991. f Dent Res1996; 75(Special Issue): 631-41.
Katz RV, Meskin LH. Testing the internal and external validity of a simplified dental caries index on an adult population. Community Dent OralEpidemiol1976; 4: 227-31.
Kingman A. A method of utilizing the subject's initial caries experience to increase efficiency in caries clinical trials. Community Dent OralEpidemiol1979; 7: 87-90
.Kitamura M, Kiyak HA, Mulligan K. Predictors of root caries in the elderly. Community Dent Oral Epidemiol1986; 14: 34-8.
Kleemola-Kujala E, Rasanen L. Relationship of oral hygiene and sugarconsumption to risk of caries in children. Community Dent OralEpidemiol1982; 10: 224-33.
Klein H. The family and dental disease. IV. Dental disease (DMF) experiencein parents and offspring. ! Am Dent Assoc 1946; 33: 735-43.
Klein H, Palmer CE. Studies on dental caries. V. Familial resemblance in the caries experience of siblings. Public Health Rep 1938; 53: 1353-64.
Klein H, Palmer CE. Community economic status and the dental problem of school children. Public Health Rep 1940; 55: 187-205.
Klein H, Palmer CE. Studies on dental caries. XII. Comparison of the caries susceptibility of the various morphological types of permanent teeth.! Dent Res 1941; 20: 203-16.
Klein H, ShirniZll T. The family and dental disease. I. DMF experience among husbands and wives. JAm Dent Assoc 1945; 32: 945-55.
Klein H, Palmer CE, Knutson IW. Studies on dental caries: I. Dental statusand dental needs of elementary school children. Public Health Rep 1938;53: 751-65.
Kohler B, Bratthall D, Krasse B. Preventive measures in mothers influence the establishment of the bacterium Streptococcus mutans in their infants. Arch Oral BioI 1983; 28: 225-31.
Kumar I, Green E, Wallace W, Bustard R. Changes in dental caries prevalence in upstate New York schoolchildren.J Public Health Dent 1991; 51:158-63.
Lawrence HP, Hunt RI, Beck JO. Three-year root caries incidence and riskl110deling in older adults in North Carolina. f Public Health Dent 1995;55: 69-78.
Lennon MA, Davies RM, Downer MC, Hull PS. Tooth loss in a 19th century British population. Arch Oral Bioi 1974; 19: 511-16.
Lingstrom P, van Houte I, Kashket S. Food starches and dental caries. CritRev Oral BioI Med 2000; 11: 366-80.
Link BG, Phelan IC Understanding sociodemographic differnces inhealth; the role of fundamental social causes [editorial]. Am f PublicHealth 1996; 86: 471-3.
Lo EC, Schwarz EC Tooth and root conditions in the middle-aged and theelderly in Hong Kong. Community Dent Oral Epidemiol1994; 22: 38J-5.
Locker D, Leake IL. Coronal and root decay experience in older adults inOntario, Canada.JPublic Health Dent 1993; 53: 158-64.
Luan W, Baelum V, Fejerskov 0, Chen X. Ten-year incidence of dental caries in adult and elderly Chinese. Caries Res 2000; 34: 205-13.
McDonald SP, Sheiham A. The distribution of caries on different tooth surfaces at varying levels of caries - a compilation of data from 18 previous studies. Community Dent Health 1992; 9: 39-48.
Macek MD, Beltran-Aguilar ED, Lockwood SA, Malvitz DM. Updated comparison of the caries susceptibility of various morphological types of permanent teeth.! Public Health DOlt 2003; 63: 174-82.
McEniery TM, Davies GN. Brisbane dental survey 1977. A comparativestudy of caries experience of children in Brisbane, Australia, over a20-year period. Community Dent Oral Epidemiol1979; 7: 42-50.
McGuire SM, Fox CH, Douglass CW, Tennstedt SL, Feldman HA. Beneath the surface of coronal caries: primary decay, recurrent decay, and failed restorations in a population-based survey of New England elders.! Public Health Dent 1993; 53: 76-82.
Machiulskiene V, Nyvad B, Baelum V. Prevalence and severity of dental caries in 12-year-old children in Kaunas, Lithuania, 1995. Caries Res1998; 32: 175-80.
Machiulskiene V, Nyvad B, Baelum V. A comparison of clinical and radiographic caries diagnoses in posterior teeth of 12-year-old Lithuanianchildren. Caries Res 1999; 33: 340-8.
Manji F, Fejerskov O. Dental caries in developing countries in relation to the appropriate use of fluoride.! Dent Res 1990; 69(Speciallssue): 733-41.
Manji F, Fejerskov 0, Baelum V, Luan W-M, Chen X. The epidemiological features of dental caries in African and Chinese populations: implications for risk assessment. In: Johnson NW, ed. Risk markers f01" oral diseases,Vol. 1, Dental caries mm・kers of high and low risk groups andindivid~lQls.Cambridge: Cambridge University Press, 1991: 62-100.
Mann I. Sugar revisited - again [editorial]. Bull WHO 2003; 81: 552.
Marcenes WS, Sheiham A. The relationship between work stress and oral health status. Sac SciMed 1992; 35: 1511-20.
Marmot M, Wilkinson RG, eds. Social determinants of health. New York:Oxford University Press, 1999.
Marmot MG, Kogenivas M, Elston MA. Social/economic status and disease. Mm Rev Public Health 1987; 8: 111-35.
Marshall TA, Levy SM, Broffitt B, Eichenberger-Gilmore IM, SlUmbo PI.Patterns of beverage consumption during the transition stage of infantnutrition.JAm Diet Assoc 2003; 103: 1350-3.
Marthaler TM, O'Mullane DM, Vrbic V. The prevalence of dental caries in Europe 1990-1995. Caries Res 1996; 30: 237-75.
Milen A. Role of social class in caries occurrence in primary teeth. Int JEpidemiol1987; 16: 252-6.
Miller WD. Agency of micro-organisms in decay of human teeth. DentCosmos 1883; 25: 1-12.
Moller IJ. Impact of oral diseases across cultures. Int Dent J 1978; 28:376-80.
Moore WJ, Corbett ME. The distribution of dental caries in ancient British populations. I. Anglo-Saxon period. Caries Res 1971; 5: 151-68. [Mollerは正しくはMøller]
Moore WJ, Corbett ME. The distribution of dental caries in ancient British populations. 11. Iron Age, Romano-British and Mediaeval periods. Caries Res 1973; 7: 139-53.
Morse OP, Holm-Pedersen P, Holm-Pedersen I, et al. Dental caries in persons over the age of 80 living in Kungsholmen, Sweden: findings from the KEOHS project. Community Dent Health 2002; 19: 262-7.
Mosha HJ, Robison VA. Caries experience of the primary dentition among groups of Tanzanian urban preschool children. Community Dent Oral Epidemiol 1989; 17: 34-7.
Mosha HI, Scheutz F. Dental caries in the permanent dentition of schoolchildren in Dar es Salaam in 1979, 1983 and 1989. Community DentOral EpidemioI1992; 20: 3!l1-2.
Mosha HI, Ngilisho LA, Nkwera H, Scheutz F, Poulsen S. Oral health status and treatment needs in different age groups in two regions of Tanzania. Community Dent Oral EpidemlOl1994; 22: 307-10.
Nicolau B, Marcenes W, Bartley M, Sheiham A. A life course approach to assessing causes of dental caries experience: the relationship betweenbiological, behavioural, socio-economic and psychological conditions and caries in adolescents. Caries Res 2003; 37: 319-26.
Nicolau B, Marcenes W, Bartley M, Sheiham A. Associations between socio-economic circumstances at two stages of life and adolescents' oral health status. JPublic Health Dent 2005; 65: 14-20.
Nuttall NM. Capability of a national epidemiological survey to predict General Dental Service treatment. Community Dent Oral Epidemiol1983; 11: 296-301.
Nuttall NM, Pitts NB, Fyffe HE. Assessment of reports by dentists of their restorative treatment thresholds. Community Dent Oral Epidemiol1993;21: 273-8.
Nyvad B, Machiulskiene V, Baelum V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions.Caries Res 1999; 33: 252-60.
Palmer lD, Pitter AFV Differences in dental caries levels between 8-yearoldchildren in Bath from different socio-economic groups. CommunityDent Health 1988; 5: 363-7.
Pappas G. Elucidating the relationships between race, socioeconomic status, and health. Am J Public Health 1994; 84: 892-3.Pattussi MP, Marcenes W, Croucher R, Sheiham A. Social deprivation income inequality, social cohesion and dental caries in Brazilian schoolchildren. Soc Sci Med 2001; 53: 915-25.
Pickerill HP. The prevention of dental caries and oral sepsis. 3rd edn.London: BaiUiere, Tindall and Cox, 1923.
Pins NB. Current methods and criteria for caries diagnosis in Europe.J Dent Educ 1993; 57: 409-14.
Pitts N. lCDAS: an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management [editorial]. Community Dent Health2004; 21: 193-8.
Pitts NB, Fyffe HE. The effect of varying diagnostic thresholds upon clinical caries data for a low prevalence group. J Dent Res 1988; 67:592-6.
Poulsen S. Dental caries in Danish children and adolescents 1988-94.Community Dent Oral Epidemio /1996; 24: 282-5.
Poulsen S, Horowitz H. An evaluation of a hierarchical method of describingthe pattern of dental caries attack. Community Dent Oral Epidemiol1974; 2: 7-1l.
Poulsen S, Scheutz F. Dental caries in Danish children and adolescents1988-1997. Community Dent Health 1999; 16: 166-70.
Riley lC, Lennon MA, ElIwood RP. The effect of water floridation and social inequalities on dental caries in 5-year-old children. Int J Epidemiol 1999; 28: 300-5.
Ringelberg ML, Matonski GM, Kimball AW. Dental caries-experience in three generations of families. l Public Health Dent 1974; 34: 174-80.
Ringelberg ML, Gilbert GH, Antonson DE, et al. Root caries and root defects in urban and rural adults: the Florida Dental Care study. JAmDent Assoc 1996; 127: 885-91.
Rugg-Gunn AJ, Hackett AF, Appleton DR, jenkins GN, Eastoe lE. Relationship between dietary habits and caries increment assessed over two years in 405 English adolescent school children. Arch Oral Bioi1984; 29: 983-92.
Russell AL. Dental caries and nutrition in Lebanon. J Dent Res 1966; 45:957-63.
Salonen L, AJlander L, Bratthall 0, et al. Oral health status in an adult Swedish population. Prevalence of caries. A cross-sectional epidemiological study in the Northern AJsvorg county. Swed Dent J 1989; 13:111-23.
Sardo lnfirri J, Bannes DE. Epidemiology of oral diseases; differences innational problems. Int Dent J 1979; 29: 183-90.
Schamschula RG, Adkins BL, Barmes DE, Charlton G, Davey BG. WHOstudy of dental caries etiology in Papua New Guinea. WHO Offset Publication No. 40. Geneva: WHO, 1978.
Sheiham A, Watt RB. The common risk factor approach: a rational basis for promoting oral health. Community Dent Oral Epidemiol 2000; 28:399-406.
Sheiham A, Maizels I, Maizels A. New composite indicators of dental health. Community Dent Health 1987; 4: 407-14.
Slade GD, Spencer AI, Gorkic E, Andrews E. Oral health status and treatment needs of non-institutionalized persons aged 60+ in Adelaide, South Australia. Aust Del1t J 1993; 38: 373-80.
Speechley M, lohnston DW. Some evidence from Ontario, Canada, of a reversal in the dental caries decline. Caries Res 1996; 30: 423-7.
Spencer AJ, Davies M, Slade G, Brennan D. Caries prevalence in Australasia.1nl Dent J 1994; 44(Suppll): 415-23.
Stamm jw. Is there a need for dental sealants? Epidemiological indications in the 1980s. J Dent Educ 1984; 48: 9-17.
Stamm lW, Banting DW, lmrey PB. Adult root caries survey of two similar ommunities with contrasting natural water fluoride levels. JAmDem Assoc 1990; 120: 143-9.
Stecksen-Blicks C, Arvidsson S, Holm A-K. Dental health, dental care, anddietary habits in children in different parts of Sweden. Acta Odor/tolScand 1985; 43: 59-67.
Steele lG, Sheiham A, Marcenes W, et al. Clinical and behavioural riskindicators for root caries in older people. Gerodontology 2001; 18:95-101.Stookey GK, Sergeant lW, Park KK, lackson RD, Drook CA. Prevalence of dental caries in Indiana school children: results of 1982 survey. PediatrDent 1985; 7: 8-13.
Sundin B, Birkhed D, Granath L. Is there not a strong relationship nowadays between caries and consumption of sweets? Swed Dent J 1983; 7:103-8.
Sundin B, Granath L, Birkhed D. Variation of posterior approximal caries incidence with consumption of sweets with regard to other caries related actors in 15-18 year-olds. Community Dent Oral EpidemioI1992;20: 76-80.
Syme SL, Berkman LF. Social class, susceptibility, and sickness. Am JEpidemiol1976; 104: 1-8.
Szpunar SM, Eklund SA, Burt BA. Sugar consumption and caries risk in schoolchildren with low caries experience. Community Dent OralEpidemiol1995; 23: 142-6.
Truin GJ, Konig KG, BronkhorSI EM, Frankenmolen F, Mulder J, van'tHof MA. Time trends in caries experience of 6- and 12-year-old children of different socioeconomic status in The Hague. Cartes Res 1998;32: 1-4.
US Department of Health and Human Services, National Center for Health Statistics. Third National Health and Nutrition Examination Survey, 1988-94. Public Use Data File No. 7-0627. Hyattsville, MD: CDC, 1997.
US Public Health Service, National Center for Health Statistics. Decayed, missing, and filled teeth in adults, United States, 1960-1962. PHSPublication No. 1000, Series 11, No. 23. Washington, DC: Government Printing Office, 1967.
US Public Health Service, National Center for Health Statistics. Decayed ,missing, and filled teeth among children; United States. DHEW Publication No. (HSM) 72-J 003, Series 11, No. 106. Washington, DC:Government Printing Office, 1971.
US Public Health Service, National Center for Health Statistics. Basic dataon dental examination findings of persons aged 1-74 years; United States. DHEW Publication No. (PHS) 79-1662, Series 11, No. 214. Washington,DC: Government Printing Office, 1979.
US Public Health Service, National Center for Health Statistics. Decayed ,missing, and filled teeth among persons 1-74 years, United States197/-1974. DHHS Publication No. (PHS) 81-1678, Series 11, No. 223.Washington, DC: Government Printing Office, 1981.
US Public Health Service, National Institute of Dental Research. The prevalence of dental caries in United States children, 1979-80. NIH Publication No. 82-2245. Washington, DC: Government Printing Office, 1981.
US Public Health Service, National Institute of Dental Research. Dentaltreatment needs of United States children. NIH Publication No. 83-2246.Washington, DC: Government Printing Office, 1982.
US Public Health Service, National Institute of Dental Research. Oral health of United States adults; national findings. NIH Publication No.87-2868. Washington, DC: Government Printing Office, 1987.
US Public Health Service, National Institute of Dental Research. Oralhealth of United States children. NIH Publication No. 89-2247.Washington, DC: Government Printing Office, 1989.
Vehkalahti MM. Paunio IK. Occurrence of root caries in relation to dental health behavior. J Dent Res 1988; 67: 911-14.
Von del' Fehr FR, Loe H, Theilade E. Experimental caries in man. CariesRes 1970; 4: 131--48.
Wallace JS. The cause and preve'ltion of decay in teeth. 2nd edn. London:Churchill, 1902.
Watt RG, Dykes J, Sheiham A. Preschool children's consumption of drinks:implications for dental health. Community Dent Health 2000; 17: 8-13.
Whelton HP, Holland TJ, O'MuUane DM. The prevalence of root surfacecaries amongst Irish adults. Gerodontology 1993; 10: 72-5.
World Bank. http: www.worldbank.orgldata!countryclass!classgroups.htm.accessed 23 August 2005.
World Health Organization. A guide to oral health epidemiological investigations.Geneva: WHO, 1979.
World Health Organization. Planning oral health services. WHO OffsetPublication No. 53. Geneva: WHO, 1980.
World Health Organization. Oral health surveys; basic methods, 4th edn.Geneva: WHO, 1997.
World Health Organization. Caries for 12-year-olds by country/area.http://www.whocollab.odont.lu.se/countriesalphab.html; accessed 18December 2003.
World Health Organization. The Significant Caries Index (SiC).http://www.whocollab.od.mah.se/expllsic.html: accessed 24 August,2005.
Figure 8.1-13
Figure 8.1 The simple matrix that is the core of all epidemiological investigations.
Figure 8.1 疫学調査の中核を示す、簡単なマトリックス。
Figure 8.2 Mean DMFT scores by age in a Kenyan population, recorded for inclusion and exclusion of enamel caries (non-cavitated).
Figure 8.2 Kenyanの集団における、年齢別DMFTスコアの平均値。(齲窩のない)エナメル質齲蝕の含除を明示。
(Source: Manji et al., 1989.)
Figure 8.3 Caries then and now: DMFT scores for 12-year-old children from various surveys in high-income countries (as defined by the World Bank) during the
period 1979-1987, and again during the period 1993-2002.
Figure 8.3 過去と現在の齲蝕。12歳児のDMFTスコア。1979-1987年と1993-2002年の(世界銀行の定義による)高所得国家における調査より。
(Source: World Health Organization, Caries for 12-year-alds by country/area.)
Figure 8.4 Caries then and now: DMFT scores for 12-year-old children from various surveys in upper middle- and lower middle-income countries (as defined by
the World Bank) during the period 1983-92, and again during the period 1994-2001.
Figure 8.4 過去と現在の齲蝕。12歳児のDMFTスコア。1983-92年と1994-2001年の(世界銀行の定義による)中高所得国家と中低所得国家における調査より。
(Source: World Health Organization, Caries for 12-year-olds by country/area.)
Figure 8.5 Mean DMFT scores in children aged 13- 14 years in nine communities in six countries.
Figure 8.5 6つの国の9つの地域における13-14歳児のDMFTスコアの平均。
(Source: Second International Collaborative Study, Chen et al., 1997.)
Figure 8.6 Decline in DMFT scores in three children's age groups between two national surveys, USA, 1988-94 and 1999-2002.
Figure 8.6 1988-94年と1999-2002年のUSAの全国調査の間に生じたDMFTスコアの減少。
(Source: Beltran-Aguilar et al., 2005.)
Figure 8.7 Decline in mean DMFS scores in six cohorts of 15-year-old children in Tamworth, Australia, over a 25-year period from 1963 to 1988.
Figure 8.7 AustraliaのTamworthにおける15歳児の6つの集団における平均DMFSスコアの減少。1963-1988年の25年を追跡。
Tamworth has fluoridated its drinking water since 1963.
Tamworthは、1963年から水道水フッ化物添加を実施している。
(Source: Barnard, 2005.)
Figure 8.8 Prevalence of caries in 5-year-old Danish schoolchildren (primary dentition), and in 15-year-old schoolchildren (permanent dentition), 1988-2005.
Figure 8.8 1988-2005年の5歳児の学童(乳歯)と、15歳児の学童(永久歯)の有病割合。
(Prevalence defined as the presence of at least one obvious cavity, or restoration or extraction due to caries.)
(最低1つの明確な齲窩あるいは齲蝕による修復、抜歯の存在として定義された有病割合)
(Source: Danish National Board of Health, Copenhagen, 2006.)
Figure 8.9 Trends in caries experience in the primary dentition in Danish 5-year-old children between 1988 and 2005.
Figure 8.9 1988-2005年の間のDanishの5歳児における乳歯の齲蝕経験の傾向。
(Source: Danish National Board of Health, Copenhagen, 2006.)
Figure 8.10 Distribution of mean DMFS values in US schoolchildren, aged 5-17 years, in a national survey in 1979-1980 and in another national survey in 1988-1994.
Figure 8.10 1979-1980年と1988-1994年のUSの学童5-17歳児の全国調査における、平均DMFS値の分布。
(Source: US Public Health Service, National Institute of Dental Research, 1981; US Department of Health and Human Services, National Center for Health Statistics, 1997.)
Figure 8.11 Prevalence of carious or restored root lesions in US adults in two national surveys, one in 1988-1994 and the other in 1999-2002.
Figure 8.11 1988-1994年と1999-2002年の2度のUSの成人の全国調査における、修復済みを含めた、歯根病巣の有病割合。
(Source: Beltran-Aguilar et al., 2005.)
Figure 8.12 Mean DMFS scores for 15-year-old children at three socioeconomic levels in the United States, 1988-1994.
Figure 8.12 1988-1994年のUSにおける3つの社会経済的水準で分けた、15歳児の平均DMFSスコア。
(Source: US Department of Health and Human Services, 1997. Reprinted with permission of Elsevier from Burt & Eklund, The dentist, dental pradice and the community. Elsevier, Philadelphia, PA; p. 244.)
Figure 8.13 Decline in mean DMFS scores in children aged 6-19 years between 1988-1994 and 1999-2002, as seen in three levels of poverty status as defined by the US federal government.
Figure 8.13 US連邦政府により定義された貧困状態の3つの水準でわけた、6-19歳児の平均DMFSスコア。1988年と1999年。
(US government’s poverty guidelines: http://aspe.cos.dhhs.gov/poverty/06poverty.shtml; accessed 14 March 2006.)
The green bars indicate the highest SES groups.
緑のバーは、最も高いSES集団を示している。
Figure 8.1-13 拡大図